

Austin Postoperative Malpractice Lawyer
Written by: Hastings Law Firm | Reviewed by: Gabe Sassin | Updated: May 6, 2026
Postoperative malpractice can happen when recovery care falls below the accepted medical standard and a preventable injury follows. Patients may be left with worsening symptoms, unclear explanations, and serious complications that could have been addressed with timely monitoring and treatment. Common concerns involve missed warning signs in the recovery room, untreated infections, medication mistakes, and surgical site errors that lead to lasting harm or fatal outcomes. If you or a loved one were harmed or worse due to postoperative malpractice in Austin, Texas, contact Hastings Law Firm for a free, confidential case review.
Trusted Austin Medical Attorneys for Surgical Recovery Negligence Claims
What You Should Know About Post-Surgical Monitoring Negligence Claims in Austin:
- Long term harm can follow when post surgical warning signs are missed during close monitoring in the hours and days after surgery.
- Options can be limited when a poor outcome is framed as a known risk even though negligence can still exist when the response to complications is not reasonable and timely.
- Severe outcomes can result when infections are not recognized or treated promptly, including organ failure, amputation, or wrongful death.
- Additional surgery and extended recovery can be required when retained foreign objects are left inside the body after surgery.
- Catastrophic injury can occur when recovery room monitoring fails to detect breathing or cardiac distress soon enough.
- Recovery can be reduced in Texas when non economic damages are capped even if economic losses like medical bills and lost wages are not capped.
- Filing options can be lost if Texas timing rules are missed, including situations where symptoms appear long after surgery.
- Case outcomes can hinge on what the medical record shows about monitoring, lab results, medication administration, and discharge stability.

A Healthcare Focused Law Firm
When recovery after surgery takes a turn you were not expecting, it can be difficult to know whether what you are experiencing is a normal complication or something that should not have happened. That uncertainty is made worse when the people you trusted with your care do not seem to have clear answers.
At Hastings Law Firm, we focus exclusively on medical malpractice. Our team of attorneys, former defense lawyers, and in-house medical professionals investigates postoperative injuries to determine whether the care you received fell below the accepted medical standard. As Austin postoperative malpractice attorneys, we can review what happened, explain your options, and help you understand whether you have a case. Consultations are confidential, and you pay nothing unless we recover compensation on your behalf.
Understanding Postoperative Malpractice and Surgical Errors
Postoperative malpractice occurs when a healthcare provider fails to meet the standard of care, the level of treatment a reasonably competent professional would have provided under similar circumstances, during a patient’s recovery, resulting in preventable harm, infection, or death. Not every poor outcome after surgery is malpractice. But when a provider’s actions or inactions fall below what is medically acceptable, and a patient is injured as a result, there may be a valid legal claim.
Texas law governs medical negligence claims through Texas Civil Practice and Remedies Code Chapter 74, which sets requirements for filing, expert reports, and the legal elements a patient must prove. A postoperative malpractice lawyer must demonstrate that the provider owed a duty, breached that duty, and that the breach directly caused the patient’s injury.
The hours and days immediately following surgery are a critical window. Patients in the recovery room require close monitoring for surgical complications like bleeding, breathing difficulties, or adverse reactions to anesthesia. When medical staff fail to catch warning signs during this period, the consequences can be severe and sometimes irreversible.
Distinguishing Between Surgical Complications and Malpractice
One of the most common barriers patients face in medical malpractice cases is what we call the “White Coat Effect,” a deep-rooted tendency to trust the doctor’s explanation without question. Providers sometimes describe preventable errors as “known surgical risks,” leaving patients unsure whether they have any recourse. While patients provide informed consent acknowledging risks, this does not grant permission for negligence. The legal threshold is not whether a complication occurred, but whether the provider’s response to it was reasonable and timely.
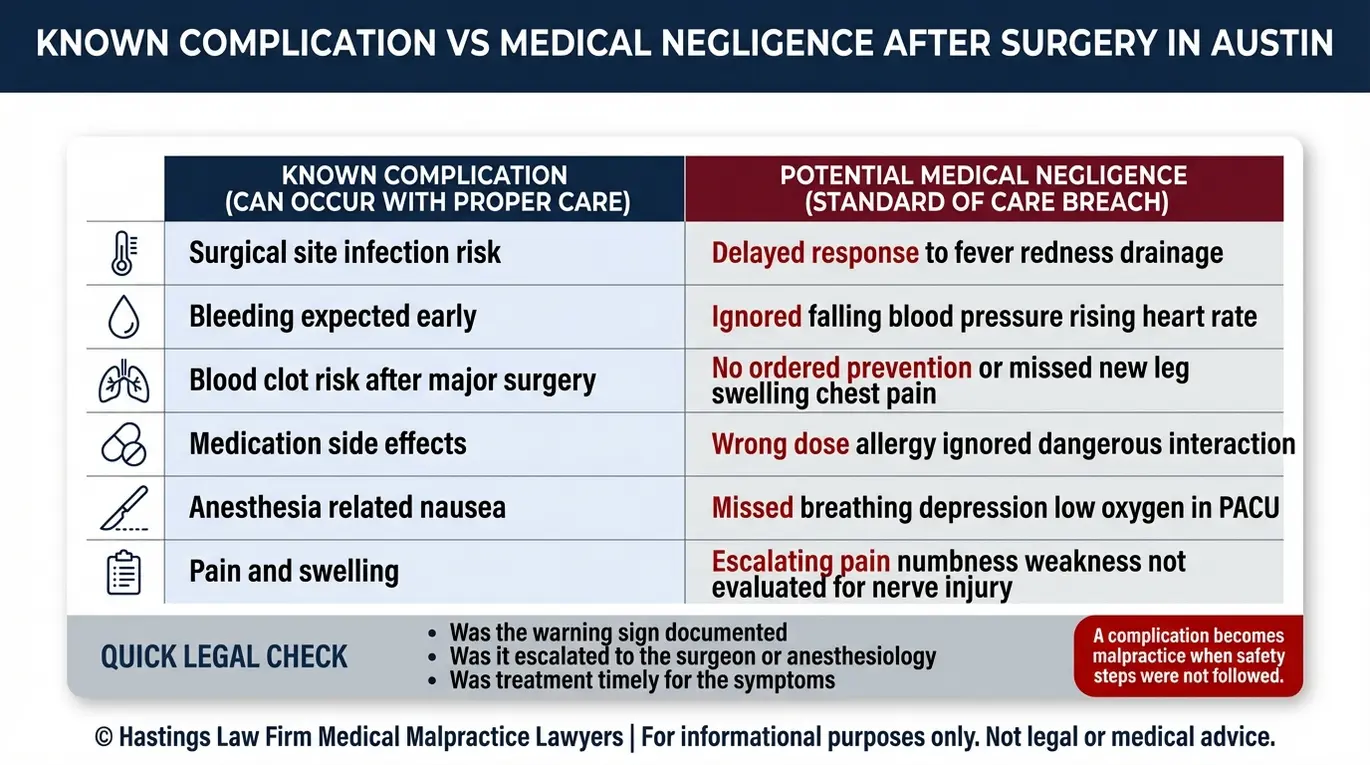
For example, infection after surgery is a recognized risk. But ignoring the signs of that infection, failing to order cultures, or delaying antibiotics is not a “risk.” It is a potential breach of duty. The distinction often comes down to what the provider did or did not do once the problem appeared.
| Known Complication | Potential Negligence |
|---|---|
| Post-surgical infection develops despite proper sterile technique | Signs of infection (fever, redness, elevated white count) are documented but not treated |
| Bleeding occurs at the surgical site | Internal bleeding goes undetected because staff fail to monitor vitals or order imaging |
| Blood clot forms after a major procedure | No DVT prophylaxis is ordered despite known risk factors |
| Patient experiences pain during recovery | Complaints of severe, worsening pain are dismissed without further evaluation |
| Swelling near the incision site | Wound dehiscence is missed because follow-up assessments are not performed |
The question in every case is whether a competent provider, facing the same situation, would have acted differently. That is the standard we measure against, and it is what separates an unavoidable outcome from medical negligence.
Common Types of Postoperative Negligence Cases We Handle
Common postoperative negligence claims involve failure to monitor vital signs, untreated infections, mismanagement of internal bleeding, wrong-site surgery, and medication errors in the recovery room. As Austin malpractice lawyers, we see recurring patterns of breakdowns in post-surgical care that cause serious, preventable injuries.
Here are the types of postoperative negligence cases our team investigates most often:
- Hemorrhage mismanagement: Internal bleeding after surgery can be life-threatening if not caught quickly. When surgical teams fail to recognize dropping blood pressure, increasing heart rate, or abdominal distention, a treatable problem can become fatal. We review post-op monitoring records to determine whether staff responded appropriately to signs of hemorrhage.
- Medication errors: Patients recovering from surgery often receive multiple medications for pain, infection prevention, and blood pressure management. Overdoses, dangerous drug interactions, or administering a medication the patient is allergic to can cause organ damage, anaphylaxis, or cardiac arrest. These errors often trace back to charting failures or poor communication between providers.
- Deep vein thrombosis and pulmonary embolism (DVT/PE): Deep vein thrombosis and pulmonary embolism (DVT/PE), conditions where a blood clot forms in a deep vein or travels to the lungs, occur in hundreds of thousands of people each year. According to the Centers for Disease Control and Prevention, these are a leading cause of preventable hospital death. Protocols for preventing DVT, such as blood thinners and compression devices, are well established. Failure to implement them may constitute negligence.
- Wound dehiscence: Wound dehiscence, the partial or complete reopening of a surgical incision, can expose internal tissue and create a serious infection risk. It often results from inadequate closure technique or failure to identify patient risk factors before discharge.
- Nerve damage and organ perforation: Injuries to surrounding nerves, blood vessels, or organs during surgery that go unrecognized in the postoperative period can cause lasting pain, loss of function, or the need for additional operations.
As postoperative negligence attorneys, our role is to trace the injury back to the specific breakdown in care. We examine the surgical notes, nursing logs, and recovery room records to identify where the standard of care was not met.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Austin courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Legal Liability for Hospital Acquired Infections and Sepsis
Hospitals may be held liable for infections like MRSA or sepsis if they result from non-sterile environments, contaminated equipment, or a failure to diagnose and treat symptoms promptly. A hospital-acquired infection (HAI), an infection a patient develops during or after receiving treatment in a healthcare facility that was not present at the time of admission, often signals a breach in safety protocols.
Sepsis, the body’s extreme and often deadly response to an infection, can progress from manageable to fatal in a matter of hours. Early symptoms include fever, elevated heart rate, confusion, and rapid breathing. When post-surgical staff fail to recognize these signs or delay treatment, sepsis can lead to organ failure, amputation, or wrongful death.
Liability in infection cases typically centers on one of three failures. The first is a breakdown in sterile technique. This might involve surgical teams using non-sterile instruments, failing to scrub in properly, or neglecting environmental cleaning, which introduces bacteria directly into the vulnerable surgical site. The second is a failure to diagnose, where providers overlook or dismiss classic signs of infection in a patient who has just undergone surgery. The third is delayed treatment, where the infection is eventually identified but antibiotics or surgical intervention are not ordered quickly enough.
As post-surgical malpractice attorneys, proving these cases requires detailed review of the hospital’s infection control policies, nursing assessments, lab results, and medication administration records. Our in-house medical staff, including nurse practitioners and board-certified patient advocates, know exactly what to look for in these records because they previously worked inside hospital systems. We also work with infectious disease specialists from our national expert network to evaluate whether the misdiagnosis of post-op symptoms fell below the accepted standard.
Surgical Site Errors and Retained Instruments
Retained foreign objects, such as sponges, clamps, or needles left inside a patient’s body after surgery, are considered “never events,” meaning they should never occur under proper surgical protocols, and they provide strong evidence of negligence in a malpractice lawsuit. An unintentionally retained foreign object (URFO), any item inadvertently left in a patient during a surgical procedure, is a serious error. Research published by PubMed Central has documented that these events continue to occur despite established counting and verification procedures.
In the context of Austin surgical error claims, the consequences for patients are severe. Retained instruments can cause internal infection, bowel or bile duct perforation, and chronic pain, often requiring additional surgery. This physical toll is compounded by the financial burden of extended hospital stays and lost time at work.
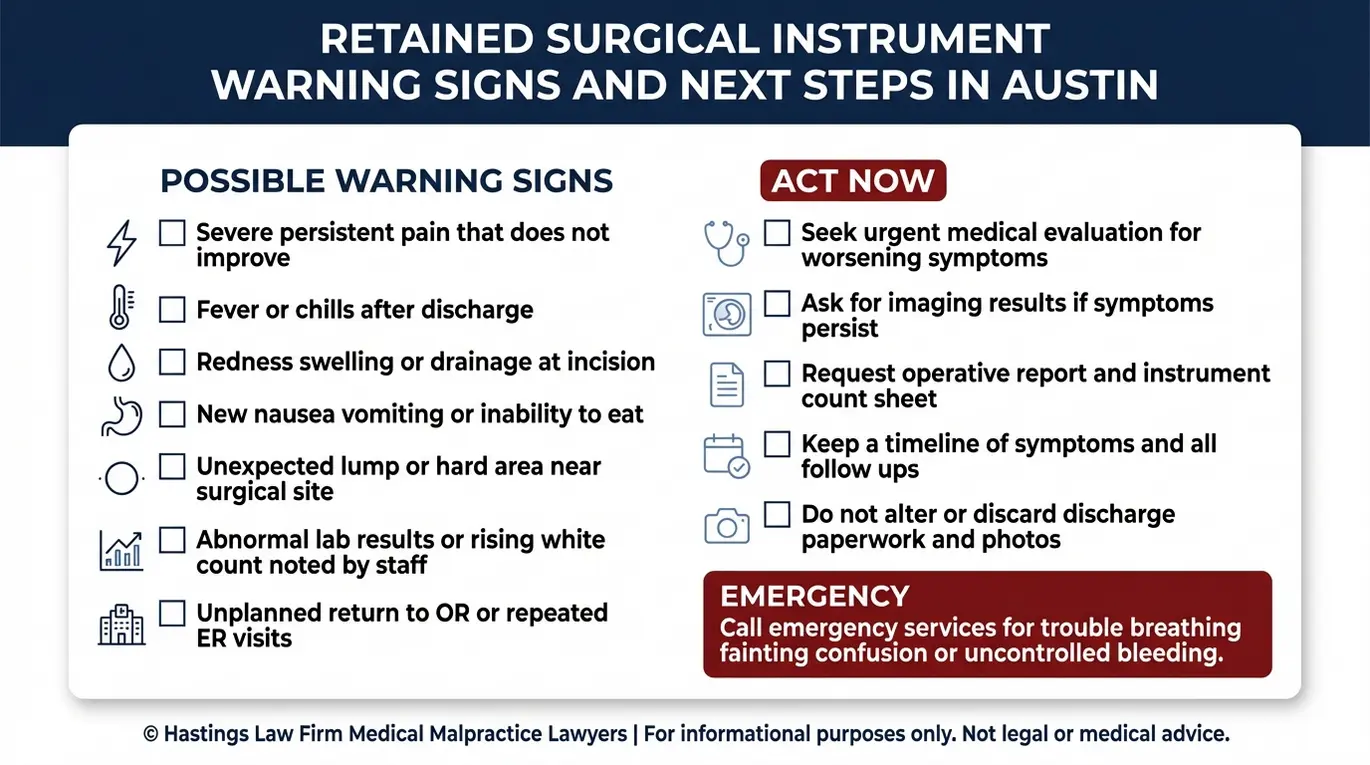
If you suspect a retained surgical instrument or experience unexplained symptoms after surgery, watch for these warning signs:
- Persistent or worsening pain at the surgical site with no clear explanation
- Recurring infections or fevers that do not respond to antibiotics
- Imaging results that reveal an unexpected foreign body
- Gastrointestinal symptoms such as nausea, vomiting, or obstruction following abdominal surgery
- A second surgeon identifies an object during a later, unrelated procedure
A lawyer for surgical errors involving retained instruments can often rely on a legal principle called res ipsa loquitur, meaning “the thing speaks for itself.” Because sponges and clamps do not end up inside a patient without someone’s error, the burden of explanation shifts toward the surgical team.
The Discovery Rule for Symptoms Appearing Years Later
In Texas, medical malpractice claims generally must be filed within two years under the Texas Medical Liability Act. In surgical error cases, retained objects present a unique problem: patients sometimes do not learn about the object for months or even years after surgery. Texas law addresses this through the discovery rule, which may allow the statute of limitations, or the legal deadline for filing a claim, to begin running from the date the patient knew about the retained object. However, this extension is not unlimited, so early legal consultation is important.
Failure to Monitor Patients in the Recovery Room
Medical staff in the PACU, or Post-Anesthesia Care Unit (the monitored recovery area where patients are observed immediately after surgery), have a duty to continuously track vital signs. Failure to detect respiratory distress, cardiac events, or other complications during this period constitutes negligence.
Post-surgical monitoring in Texas facilities exists for a specific reason: patients emerging from anesthesia are at elevated risk for airway obstruction, dangerously low oxygen levels, and adverse drug reactions. Nurses and anesthesiologists in this unit are responsible for monitoring breathing, heart rate, blood pressure, oxygen saturation, and level of consciousness at regular intervals. Standardized tools, such as the Aldrete Discharge Scoring system studied at UNH Scholars’ Repository, help determine when a patient is stable enough to leave the recovery area.
When a failure to monitor occurs, the results can be devastating. Hypoxia, a condition in which the body or brain does not receive enough oxygen, can cause permanent brain damage within minutes. Anesthesia errors that suppress a patient’s ability to breathe independently require immediate intervention.
If a PACU nurse is assigned too many patients, is distracted, or simply does not check on a patient frequently enough, a recoverable situation can become a catastrophe. Premature discharge is another critical error; sending a patient home while they are still under the effects of anesthesia or unstable increases the likelihood of a medical emergency occurring away from immediate help.
As recovery room negligence attorneys, we examine staffing records, nursing notes, and monitoring logs to determine whether the care team met its obligations. We also evaluate whether the patient was discharged from the PACU prematurely, before meeting the clinical criteria for safe transfer, and whether discharge instructions provided adequate guidance for recognizing warning signs at home.
How We Prove Postoperative Medical Negligence
Proving negligence requires clear evidence that the provider breached the standard of care, typically established through medical records, expert witness testimony, and a direct link between the provider’s conduct and the patient’s injury. Under the Texas Medical Liability Act (codified in Texas Civil Practice and Remedies Code § 74.351), a plaintiff must serve an expert report within 120 days after the defendant’s original answer is filed, making early investigation essential.
Here is how we build a postoperative negligence case:
- Medical record collection and review. We obtain the complete surgical record, including operative notes, anesthesia logs, nursing charts, lab results, and medication administration records. Our founder, Tommy Hastings, is board-certified in personal injury trial law, a distinction held by fewer than 2% of Texas attorneys. Our in-house medical staff, which includes nurse practitioners and board-certified patient advocates, reviews these documents for gaps or signs that protocols were not followed.
- Expert evaluation. We consult with qualified medical experts from our national network who practice in the same specialty as the provider in question. These experts assess whether the care provided fell below the accepted standard and prepare the required written report.
- Establishing causation. It is not enough to show that a provider made an error. We must also demonstrate that the error, and not a pre-existing condition or unavoidable complication, directly caused the injury. This involves a detailed medical reconstruction of the patient’s timeline, from the operating room through discharge and beyond.
- Building the case for trial. Every case we accept is prepared from the outset as though it will go before a jury. This trial-ready approach strengthens our position whether the case resolves through negotiation or requires a courtroom presentation.

Damages Recoverable for Surgical Complications in Texas
Patients harmed by surgical malpractice in Texas may recover economic damages for medical bills and lost wages, as well as non-economic damages for pain and suffering, subject to state caps.
Economic damages cover the measurable financial losses tied to the injury. These include:
- Past and future medical costs, including corrective surgeries, rehabilitation, and ongoing treatment
- Lost wages and lost earning capacity if the injury affects the patient’s ability to work
- Home care, assistive devices, and other out-of-pocket costs
Non-economic damages address the less tangible harms: physical pain, emotional distress, loss of enjoyment of life, and disfigurement. Under Texas Civil Practice and Remedies Code § 74.301, non-economic damages in medical malpractice cases are subject to a non-economic damages cap, currently at $250,000 per claimant against all physicians or individual providers and up to $250,000 per claimant against each healthcare institution, with a maximum of $500,000 across all institutions. Economic damages are not subject to a cap.
In cases involving wrongful death, surviving family members may pursue a separate claim for loss of companionship, mental anguish, and the financial support the deceased would have provided. An Austin medical malpractice lawyer can help determine which categories of damages apply to your specific situation and what the realistic recovery range may look like.
Contact the Austin Surgical Error Attorneys at Hastings Law Firm Today for Help
If you or a loved one suffered a preventable injury during recovery from surgery, you deserve answers. At Hastings Law Firm, our mission is to restore trust for patients who feel let down by the healthcare system and to hold negligent providers accountable so the same mistakes are not repeated.
We focus exclusively on medical malpractice. Our team includes former hospital defense attorneys, in-house nurse consultants, and a national network of medical experts, all working together to investigate what happened and determine whether your care fell short of the standard.
As your Austin postoperative malpractice attorneys, we handle every step of the legal process while you focus on healing. There are no upfront fees or costs. You pay nothing unless we secure a recovery on your behalf under a contingency fee agreement.
Contact us today for a free, confidential case evaluation. We can review your records, explain your options, and help you take the next step toward the truth.
Frequently Asked Questions About Postoperative Malpractice in Austin

Key Postoperative Malpractice Terms:
- Wound dehiscence
- The partial or complete separation of the layers of a surgical incision after surgery. In a postoperative negligence case, wound dehiscence may indicate improper closure technique, failure to address infection, or inadequate monitoring of the surgical site during recovery.
- Deep vein thrombosis / pulmonary embolism (DVT/PE)
- Deep vein thrombosis (DVT) is a blood clot that forms in a deep vein, usually in the leg, while pulmonary embolism (PE) occurs when that clot breaks loose and travels to the lungs, blocking blood flow. These conditions are serious postoperative complications that can be fatal if not prevented or treated promptly. In malpractice cases, DVT/PE may result from a hospital’s failure to use blood-thinning medication, compression devices, or early mobilization after major surgery.
- Hospital-acquired infection (HAI)
- An infection that a patient develops while receiving treatment in a hospital or healthcare facility, which was not present or incubating at the time of admission. In postoperative malpractice claims, hospital-acquired infections may result from unsterile surgical instruments, contaminated environments, or failure to follow proper hygiene protocols, and can lead to serious complications including sepsis.
- Sepsis
- A life-threatening condition that occurs when the body’s response to an infection causes widespread inflammation and can lead to tissue damage, organ failure, and death. Sepsis progresses rapidly and requires immediate medical intervention. In malpractice cases, sepsis claims often involve a hospital’s failure to recognize early warning signs such as fever, elevated heart rate, or altered mental status, or failure to treat an infection aggressively enough to prevent it from spreading.
- Unintentionally retained foreign object (URFO)
- A surgical instrument, sponge, needle, or other medical item accidentally left inside a patient’s body after an operation is closed. This error typically requires additional surgery to remove the object and can cause serious complications including infection, pain, and internal injury. In medical malpractice law, a retained foreign object is considered strong evidence of negligence because proper counting procedures should prevent it.
- Never event
- A serious, preventable medical error that should never occur in a healthcare setting, such as operating on the wrong body part, leaving a surgical instrument inside a patient, or performing the wrong procedure. These events are considered indefensible mistakes that indicate a clear breach of the standard of care, making them particularly strong grounds for a medical malpractice claim.
- Post-Anesthesia Care Unit (PACU)
- The recovery room where patients are closely monitored immediately after surgery while waking from anesthesia. PACU nurses and anesthesiologists track vital signs, pain levels, and potential complications during this critical period. In postoperative malpractice cases, failure to properly monitor patients in the PACU can lead to undetected breathing problems, medication errors, or premature discharge before the patient is stable.
- Hypoxia
- A condition in which the body or a region of the body does not receive adequate oxygen supply. After surgery, hypoxia can occur due to anesthesia complications, airway obstruction, or inadequate breathing monitoring in the recovery room. Even brief periods of hypoxia can cause permanent brain damage or death, making proper monitoring in the PACU critical to patient safety.
- Texas Civil Practice and Remedies Code Chapter 74 | Texas Legislature Online
- Data and Statistics on Venous Thromboembolism | CDC
- Unintentionally retained foreign objects URFOs Adverse events influenced by the pandemic A case series and literature review | PubMed Central
- Aldrete Discharge Scoring Appropriate for Post Anesthesia Phase I | UNH Scholars’ Repository
- Texas Civil Practice and Remedies Code, Chapter 74.051 | Texas Legislature Online
- Texas Civil Practice and Remedies Code Section 74.301 | Texas Legislature Online
- Licensee Complaint Form | Texas Medical Board
Get Answers Today
If you think that medical negligence, a dangerous drug, or a failed medical product caused harm to you or someone you love, our team is standing by to offer guidance. We’ll explain your options under current laws and help you move forward with clarity and understanding. Case reviews are free and 100% confidential.
