

Texas Uterine Rupture Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
A uterine rupture during labor is a catastrophic obstetric emergency that can harm both mother and baby. When warning signs are missed, high risk deliveries are mismanaged, or an urgent cesarean section is delayed, families can face severe bleeding, emergency surgery, permanent infertility, brain injury, or worse. Understanding common red flags, high risk scenarios such as VBAC and labor induction, and the importance of rapid response can clarify how preventable errors happen. If you or a loved one were harmed or worse due to uterine rupture during labor in Texas, contact Hastings Law Firm for a free, confidential case review.
Top-Rated Legal Representation for Catastrophic Birth Injuries in Texas
What You Should Know About Hysterorrhexis & Hemorrhage Claims in Texas:
- Life changing maternal and infant injuries can follow a uterine rupture when warning signs are missed or emergency delivery is delayed.
- Permanent brain damage or death can result when a rupture disrupts oxygen supply and the response is not rapid.
- A full rupture can create catastrophic bleeding and shock for the mother, sometimes requiring emergency hysterectomy.
- The difference between uterine rupture and uterine dehiscence can affect how severity and provider response are evaluated.
- Preventable rupture allegations often focus on VBAC management and the use of labor inducing drugs such as Pitocin.
- Recovery options in Texas can be lost if filing time limits are missed.
- Compensation can include economic damages for medical costs and long term care and non economic damages for pain suffering and impairment.
- Non economic damages in Texas are limited by caps, while economic damages are not capped.
- Disputes often turn on whether fetal monitoring and clinical documentation show early distress that required immediate action.
- Key records such as fetal monitoring strips and operative reports can be central when evaluating what happened during delivery.

A Healthcare Focused Law Firm
A uterine rupture during labor is one of the most dangerous obstetric emergencies a mother and baby can face. When it happens because a medical team failed to recognize the warning signs, mismanaged a high-risk delivery, or delayed a necessary cesarean section, the outcome can be devastating. Brain injuries, emergency hysterectomies (the surgical removal of the uterus), and the loss of a child are not risks families should bear because of preventable medical errors.
If you or your baby suffered serious harm, you deserve answers about what went wrong and who is responsible. At Hastings Law Firm, our team includes attorneys, nurse consultants, and former hospital defense lawyers. Founder Tommy Hastings is board-certified in Personal Injury Trial Law, a qualification held by fewer than 2% of attorneys in Texas.
A Texas uterine rupture lawyer at our firm can review your medical records and explain your legal options. Contact us for a free, confidential case evaluation.
Understanding Uterine Rupture and Medical Liability
A uterine rupture occurs when the muscular wall of the uterus tears during pregnancy or labor, potentially expelling the fetus into the mother’s abdomen. We investigate every detail of your care to determine if medical liability exists because providers failed to recognize risk factors or delayed surgical intervention. Medical liability refers to the legal responsibility a healthcare provider has when their failure to meet safety standards causes harm.
The tear involves a complete division of all three layers of the uterus: the endometrium (inner lining), the myometrium (thick muscular layer responsible for contractions), and the perimetrium or serosa (outer membrane). When these layers give way, two life-threatening emergencies unfold at once. The mother can experience massive hemorrhage leading to hypovolemic shock, a dangerous drop in blood volume that can cause organ failure. At the same time, the baby loses its oxygen supply as the placenta separates, putting the infant at immediate risk of permanent brain damage or death.
Research in a study published in PubMed Central shows that outcomes depend heavily on how quickly the medical team identifies and responds to the rupture. This is why our team includes former hospital nurses who understand labor protocols. They analyze records to determine if the care team missed warning signs requiring an emergency response.
An experienced uterine rupture attorney examines the clinical timeline, from admission notes to fetal monitoring strips, to show whether the standard of care was met.
Rupture vs. Uterine Dehiscence
Not every uterine scar complication is a full rupture, and the distinction matters for both anatomy and legal analysis.
| Feature | Uterine Rupture | Uterine Dehiscence |
|---|---|---|
| Definition | Complete tear through all layers of the uterine wall, including the serosa (outer membrane) | Partial thinning or “window” in the scar tissue; the serosa remains intact |
| Severity | Catastrophic; immediate surgical emergency | Often less acute; may be discovered incidentally during a planned C-section |
| Fetal Risk | High; fetus may be expelled into the abdomen with complete loss of oxygen | Lower; fetal compromise is less common but still possible |
| Maternal Bleeding | Massive hemorrhage is typical | Bleeding is usually minimal |
| Legal Significance | Strong basis for malpractice if warning signs were ignored or response was delayed | May still support a claim if providers failed to identify risk factors or monitor appropriately |
Uterine dehiscence is a partial separation where the scar thins but serosa integrity is maintained. This is a less severe event. However, a dehiscence can progress to a full rupture if not identified and managed properly. Understanding this difference is essential when building a medical malpractice case because it directly affects how we show the severity of the injury and the provider’s duty to respond.

Warning Signs Doctors Must Recognize During Labor
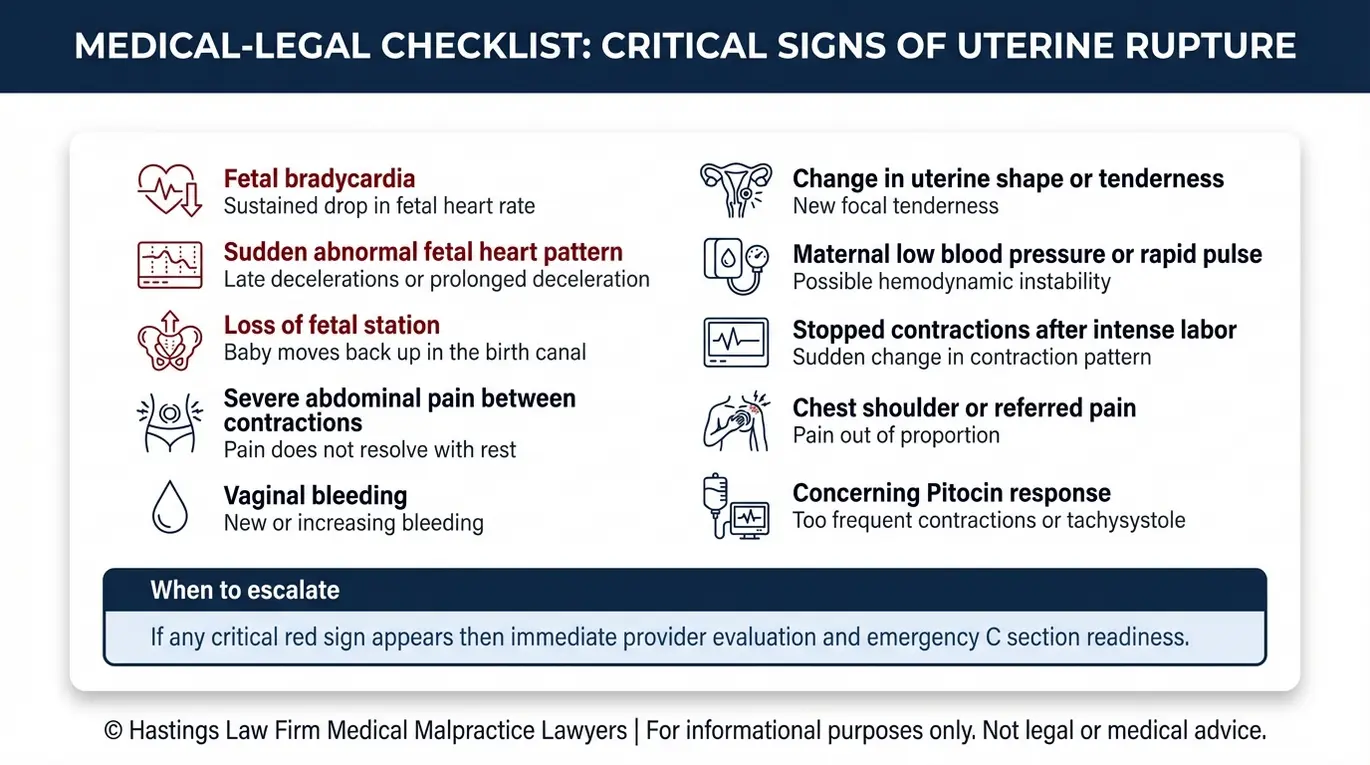
Medical providers have a legal obligation to monitor for signs of impending uterine rupture, particularly in high-risk patients. Our legal team evaluates whether the medical staff followed the accepted standard of care by identifying clinical red flags. These indicators include abnormal fetal heart rate patterns, severe abdominal pain that persists between contractions, and a sudden loss of fetal station.
Here are the clinical red flags providers are required to identify and respond to:
- Fetal bradycardia: A sudden, prolonged drop in the baby’s heart rate is the single most common sign of uterine rupture. It is present in approximately 80% of cases according to research published in PubMed on fetal heart rate changes associated with uterine rupture. This occurs because the placenta detaches from the uterine wall, cutting off the baby’s oxygen supply.
- Severe maternal pain: Sharp, tearing abdominal pain that does not resolve between contractions can signal that the uterine wall is giving way.
- Loss of fetal station: The presenting part of the baby, usually the head, recedes back up the birth canal. This happens when the baby is displaced through the uterine tear.
- Vaginal bleeding: Unexplained or sudden heavy bleeding during labor may indicate internal hemorrhage from a rupture site.
- Maternal hemodynamic instability: A rapid drop in blood pressure, elevated heart rate, or signs of shock suggest significant blood loss consistent with a ruptured uterus.
Our team obtains and analyzes fetal heart rate strips, nursing notes, and physician documentation to determine whether fetal distress warning signs were present. Our in-house nursing staff reviews the timing of each clinical event. We look for gaps between when providers should have acted and when they finally intervened.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Negligence Leading to Rupture: Pitocin and VBAC Errors
The two most common causes of preventable uterine rupture involve the mismanagement of Vaginal Birth After Cesarean (VBAC) and the improper use of labor-inducing drugs like Pitocin. Both situations create conditions where contractions can become too powerful for a scarred uterus to withstand.
Pitocin and Uterine Tachysystole
Pitocin is the synthetic form of the hormone oxytocin and is used to induce labor. When used without proper monitoring, it can cause uterine tachysystole, a condition where the uterus contracts more than five times in ten minutes. In a patient with a prior cesarean scar, these excessive contractions place enormous stress on the weakened tissue.
Research from a review published in PubMed Central on acute tocolysis for uterine tachysystole emphasizes that providers must recognize and treat tachysystole promptly. Failure to reduce the Pitocin dosage or use tocolytic medication to slow contractions can be a sign of negligence. Cervical ripening drugs, including prostaglandins like misoprostol, carry similar risks and are generally avoided in patients with a prior uterine scar.
VBAC and TOLAC Protocol Failures
A Trial of Labor After Cesarean (TOLAC) requires strict safety protocols. The standard of care typically requires that an obstetrician and anesthesiologist be immediately available throughout the labor. Hospitals that offer VBAC without the staffing and surgical resources to perform an emergency C-section within minutes are putting patients at serious risk.
The type of prior uterine incision also matters. Patients with a classical (vertical) incision face a significantly higher rupture risk than those with a low transverse incision. A malpractice claim regarding uterine rupture often centers on whether the provider properly assessed these risk factors before allowing labor to proceed.
If your medical team failed to follow these protocols, a lawyer for uterine tear cases can evaluate the records to determine if their decisions fell below accepted medical standards.
| Risk Factor | Why It Matters |
|---|---|
| Prior classical (vertical) uterine incision | Carries the highest risk of rupture during subsequent labor |
| Pitocin or prostaglandin use with a uterine scar | Increases contraction intensity on weakened tissue |
| Short inter-pregnancy interval (less than 18 months) | Scar tissue may not have fully healed |
| No surgeon immediately available during TOLAC | Delays emergency delivery if rupture occurs |
| Multiple prior cesarean deliveries | Each surgery thins and weakens the uterine wall |
Emergency Response: The Decision-to-Incision Standard
When a uterine rupture occurs or is strongly suspected, the standard of care generally requires delivery of the baby within 30 minutes to prevent permanent brain damage or death. Delays beyond this window are often the central issue in a medical malpractice lawsuit.
The decision-to-incision interval is the time measured from the moment a provider decides an emergency cesarean section is necessary to the moment the surgical incision is made. According to research from the University of San Francisco on standardizing decision-to-incision intervals, this metric is a recognized benchmark for evaluating emergency obstetric response. Every minute that passes increases the baby’s risk of hypoxic-ischemic encephalopathy (HIE). This is a type of brain damage caused by oxygen deprivation that can lead to cerebral palsy and lifelong cognitive impairment.
A timeline of negligence in these cases often follows this pattern:
- Start of Distress: Fetal monitoring shows severe bradycardia or maternal pain spikes.
- Standard of Care: The medical team calls a “stat” C-section; delivery occurs within 30 minutes.
- Negligent Delay: The team fails to mobilize, leading to prolonged hypoxia, or a lack of oxygen to the brain, and catastrophic injury.
The surgical response to a rupture often involves an emergency C-section to deliver the baby and an emergency hysterectomy to save the mother’s life.
A ruptured uterus attorney in Texas will examine the timeline of events closely to identify any breach of duty. We ask when fetal monitoring first showed signs of distress and when the provider decided to proceed with an emergency delivery.
We also look at how long it took to get the patient into the operating room and whether an anesthesiologist was on site. Staffing failures are a common source of liability. When a hospital allows a high-risk labor without an obstetrician and anesthesiologist immediately available, critical minutes are lost. This can turn a treatable complication into a tragedy.
Damages for Maternal Injury and Infant Brain Damage
Families affected by uterine rupture in Texas can recover both economic damages for measurable financial losses and non-economic damages for pain, suffering, and physical impairment. Because these cases often involve permanent injuries to the mother, the baby, or both, compensation for uterine rupture can reach multi-million-dollar figures. Economic damages represent financial losses like medical bills, while non-economic damages cover intangible losses like emotional distress.
Maternal Damages:
- Medical costs for emergency surgery, blood transfusions, and ongoing care
- Permanent infertility if an emergency hysterectomy, the surgical removal of the uterus, was required to control life-threatening postpartum hemorrhage (severe bleeding after delivery)
- Psychological trauma, including PTSD, anxiety, and depression
- Lost wages and diminished earning capacity
Infant Damages:
- Lifetime life-care costs for a child diagnosed with HIE or cerebral palsy
- Specialized medical equipment, home modifications, and assistive technology
- Ongoing physical therapy, occupational therapy, and speech therapy
- Educational support and developmental services
Wrongful Death:
When a uterine rupture results in the death of the mother or the baby, surviving family members may pursue a wrongful death claim. These cases account for both the economic contributions the deceased would have made and the emotional loss suffered by the family.
We work with life-care planners and economic experts to calculate the scope of damages. Our goal is to ensure any settlement or verdict reflects the true cost of the injury.
Texas Time Limits for Filing Birth Injury Claims
In Texas, the statute of limitations generally gives parents two years from the date of injury to file a medical malpractice claim. Missing this statute of limitations can permanently bar your right to seek compensation. Consulting a Texas uterine rupture lawyer early is critical to preserving evidence and protecting your legal options.
The Two-Year Rule
A statute of limitations is the legal deadline for filing a lawsuit. Under Texas Civil Practice & Remedies Code Chapter 74, the mother’s claim for her own injuries must typically be filed within two years of the date of injury.
The Minors’ Exception
For the baby’s injury claim, Texas law provides an extended timeline. This rule acknowledges that birth-related injuries may not be fully understood until a child reaches certain developmental milestones. A minor child generally has until their 14th birthday to file suit, giving families additional time to understand the full extent of the child’s injuries as they develop.
The Statute of Repose
While the discovery rule can sometimes extend deadlines when an injury isn’t immediately obvious, Texas also imposes an absolute 10-year deadline, known as the statute of repose. Regardless of when an injury is discovered, no claim can be filed more than 10 years after the date of the negligent act.
A Texas uterine rupture lawyer at Hastings Law Firm can help ensure evidence preservation, including fetal monitoring strips and medical records, before it is lost or destroyed.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
If you or your baby suffered serious harm from a uterine rupture during delivery, you deserve to know what happened and whether medical negligence was involved. These cases require a legal team that understands both the medicine and the law, and that has the resources to hold hospitals and providers accountable.
At Hastings Law Firm, we dedicate our entire practice to medical malpractice. Our team includes former defense lawyers who know how hospitals prepare their cases and in-house nurse consultants who can read your medical records with a clinical eye. We charge no attorney fees or costs unless we recover compensation for you.
We are ready to listen to your story and help you understand your legal path forward. Contact us today for a free, confidential case evaluation.
Frequently Asked Questions About Uterine Rupture in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
