

Texas Rotational Forceps Birth Injury Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Rotational forceps delivery is a high risk assisted vaginal delivery that requires specialized skill and careful judgment. When forceps are used with excessive force, incorrect technique, or poor decision making, a baby can suffer serious injuries and a mother can experience significant pelvic trauma and lasting complications. Concerns often focus on whether fetal position and station were assessed correctly, whether fetal monitoring showed distress, and whether the delivery should have moved to a cesarean section sooner. If you or a loved one were harmed or worse due to rotational forceps delivery errors in Texas, contact Hastings Law Firm for a free, confidential case review.

Nationally Recognized Advocacy for Families Impacted by Forceps Delivery Errors
What You Should Know About Infant Rotational Forceps Injury Claims in Texas:
- Lifelong disabilities can result when rotational forceps are used with excessive force or incorrect technique.
- Severe maternal injuries can follow a traumatic rotational forceps delivery, including tearing and long term pelvic complications.
- Options can narrow when a rotational forceps attempt continues despite signs of fetal distress on electronic fetal monitoring.
- The risk of catastrophic injury can rise when vacuum extraction and forceps are both used during the same delivery.
- Preventable harm may be indicated when fetal station or fetal position was assessed incorrectly before forceps were applied.
- Recovery can be shaped by Texas limits on non economic damages even when economic damages for long term care are not capped.
- Disputes often turn on whether the physician stopped after unsuccessful pulls rather than continuing the attempt.
- Clarity about what happened can depend on objective records such as fetal heart rate strips and delivery documentation.
- Conflicting accounts can emerge when the operative report does not match nursing notes recorded during labor.
- Long term financial needs can be central when a child requires ongoing care and specialized therapies after a forceps injury.

A Healthcare Focused Law Firm
When a birth injury happens during a forceps delivery, the confusion and fear that follow can be overwhelming. You may have questions about what went wrong, whether it could have been prevented, and what options exist to protect your child’s future. These are the right questions to ask.
At Hastings Law Firm, we focus exclusively on medical malpractice, and birth injuries from operative deliveries are among the most challenging cases we handle. As a Texas rotational forceps birth injury lawyer, our team of attorneys, in-house nurse consultants, and former defense counsel investigates these cases with the medical depth they demand. If your family has been affected, we welcome the opportunity to review what happened and explain your options in a free, confidential consultation.
Understanding Rotational Forceps and Assisted Vaginal Delivery
Rotational forceps deliveries involve using specialized instruments, such as Kielland forceps, to rotate a baby’s head within the birth canal to a safer position for delivery. Assisted deliveries using instruments require high levels of physician skill to avoid injury. This type of assisted vaginal delivery is one of the most technically demanding procedures in obstetrics, and the risks it carries are significantly higher than other instrument-assisted approaches.
Kielland forceps are a specific type of obstetric forceps designed with a sliding lock and minimal pelvic curve, allowing a physician to grasp and rotate the baby’s head when it is facing the wrong direction. The goal is to turn the baby into the optimal face-down position so delivery can proceed. This is sometimes called a mid-forceps delivery because the baby’s head is still relatively high in the pelvis.
The distinction between rotational and outlet forceps matters enormously from both a medical and legal standpoint. An outlet forceps delivery is performed when the baby’s head is already visible at the perineum and no rotation is needed. The physician simply provides gentle traction to guide the baby out. A rotational forceps delivery, by contrast, requires the physician to manipulate the baby’s head through a turn of up to 90 degrees or more while it is still deep in the mid-pelvis. The margin for error is narrow, and the consequences of excessive force or incorrect technique can be severe.
| Feature | Rotational Forceps (Mid-Forceps) | Outlet Forceps |
|---|---|---|
| Risk Level | High | Lower |
| Rotation Required | Yes (up to 90°+) | None |
| Fetal Station | Mid-pelvis | Scalp visible at perineum |
| Skill Demand | Highly specialized | Standard obstetric training |
| Common Instrument | Kielland forceps | Simpson or Tucker-McLane forceps |
Not every difficult delivery warrants forceps. According to the NCBI Bookshelf overview on vacuum extraction, assisted vaginal delivery methods carry distinct risk profiles that must be weighed against the alternative of a C-section. When fetal distress is present or the baby is not progressing, the decision between forceps, vacuum extraction, and cesarean delivery is one of the most consequential a physician will make.
Strict Clinical Prerequisites for Safe Forceps Use
Before forceps can be applied, specific clinical conditions must be confirmed. These benchmarks help medical teams decide if an operative delivery is safe. Two of the most important are fetal station, which describes how far the baby’s head has descended into the pelvis, and fetal position, which refers to the direction the baby is facing. For a rotational delivery, the fetal position is typically abnormal, meaning the baby needs to be turned.
The standard of care requires the physician to accurately assess both station and position before proceeding. An electronic fetal monitor should be showing a reassuring heart rate pattern. The cervix must be fully dilated, and the physician must have confirmed the baby’s exact position. Medical records documenting these assessments are some of the first things a Texas rotational forceps injury attorney will review, because errors in judging station or position are a frequent source of preventable harm.

Common Injuries Caused by Negligent Forceps Rotation
Negligent rotation during a forceps delivery can cause skull fractures, intracranial hemorrhages, facial nerve palsy, and permanent brain damage due to oxygen deprivation. When a doctor uses too much force, the infant can suffer permanent physical harm. These injuries range from conditions that may resolve with treatment to lifelong disabilities.
Traumatic Brain Injury and Hemorrhage
The infant skull is soft and not yet fully fused, which makes it especially vulnerable to compression and shearing forces. When excessive traction or improper rotation is applied during a forceps delivery, the result can be a brain bleed. Intracranial hemorrhage, meaning bleeding inside the skull, can occur in several forms, including subdural, subarachnoid, or intraventricular hemorrhage.
A related and particularly dangerous condition is subgaleal hemorrhage, which involves bleeding between the scalp’s galea aponeurosis and the skull’s periosteum. Research published in *Obstetrics & Gynecology* on neonatal subgaleal hemorrhage has documented the association between operative vaginal delivery and this life-threatening bleeding event. A brain bleed may not always be immediately obvious at birth, making timely imaging and monitoring essential.
Nerve Damage
Forceps placed incorrectly or with excessive pressure can compress the facial nerve as it passes near the jaw, leading to facial nerve injury and, in some cases, permanent facial paralysis. The baby may be unable to close one eye, smile symmetrically, or control muscles on the affected side of the face.
Brachial plexus injuries are another serious risk, particularly when shoulder dystocia occurs alongside a forceps delivery. Shoulder dystocia is a complication where the baby’s shoulder becomes lodged behind the mother’s pubic bone. Damage to the brachial plexus nerves can result in Erb’s palsy, a condition that causes weakness or paralysis in the arm and shoulder. In severe cases, surgical intervention is required and full recovery is not guaranteed.
Oxygen Deprivation
Prolonged or repeated forceps attempts can lead to hypoxia, a condition where the baby’s brain does not receive adequate oxygen. Hypoxia during delivery is one of the leading causes of cerebral palsy and other permanent neurological conditions. Even brief periods of oxygen deprivation during the critical moments of birth can cause damage that affects motor function, cognition, and development for a lifetime.
If your child was diagnosed with any of these conditions after a forceps delivery, consulting a forceps injury lawyer in Texas can help you understand whether the injuries were preventable.
Maternal Injuries Associated with Rotational Forceps
A rotational forceps delivery involves high-risk movements that can lead to significant pelvic damage. Mothers can experience severe perineal tearing, including third-degree and fourth-degree lacerations that extend into the anal sphincter. Pelvic floor damage, bladder injuries, and long-term complications such as incontinence or pelvic organ prolapse may also result from a traumatic forceps delivery. These maternal injuries often require surgical repair and extended recovery, adding significant economic damages to any claim based on medical negligence.
Mothers may also face psychological trauma following a difficult operative delivery. The recovery period can disrupt bonding with the newborn and delay the return to work, further compounding the family’s financial and emotional stress.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Identifying Malpractice in Forceps Deliveries
Malpractice occurs when a physician attempts a rotational delivery without proper indication, applies excessive force, or fails to abandon the procedure for a C-section after failed attempts. Malpractice is a failure to meet the accepted medical standard of care. Identifying these failures requires an understanding of the clinical guidelines that govern operative vaginal delivery.
The Three-Pull Limit
The standard of care places limits on how many attempts a physician should make during an operative vaginal delivery. Clinical guidelines generally provide that if the baby does not descend meaningfully after three pulls with the forceps, the procedure should be abandoned. Continuing beyond this threshold significantly increases the risk of traumatic injury. Guidelines from CRICO’s OB Guideline 18 on Operative Vaginal Delivery reinforce the importance of defined limits and clear decision points.
The Danger of Sequential Instrument Delivery
Sequential instrument delivery, commonly called stacking, refers to switching from vacuum extraction to forceps or the reverse during the same delivery. Clinical guidance from organizations like ACOG, as summarized by Guideline Central, generally discourages this practice because the combined trauma of two different instruments dramatically increases the risk of intracranial hemorrhage and skull fracture.
This practice is dangerous because the scalp and skull are subjected to compounding forces that exceed the tolerance of the fetal head. When a birth injury lawsuit is filed, we investigate whether the physician exhausted multiple instrument types before delivering the baby. When medical records show that both a vacuum and forceps were used on the same baby, it raises immediate questions about whether the standard of care was followed.
Failure to Proceed to C-Section
One of the most common forms of medical malpractice in these cases involves the decision to attempt or continue a forceps delivery when fetal heart rate monitoring shows signs of fetal distress. If the electronic fetal monitor is displaying non-reassuring patterns, the standard of care may require the physician to move to an emergency C-section rather than persist with an operative vaginal delivery. The decision to continue with forceps despite warning signs is a central issue our team examines in these cases. We rely on expert testimony to confirm that a reasonable physician would have performed a cesarean section under the same circumstances.
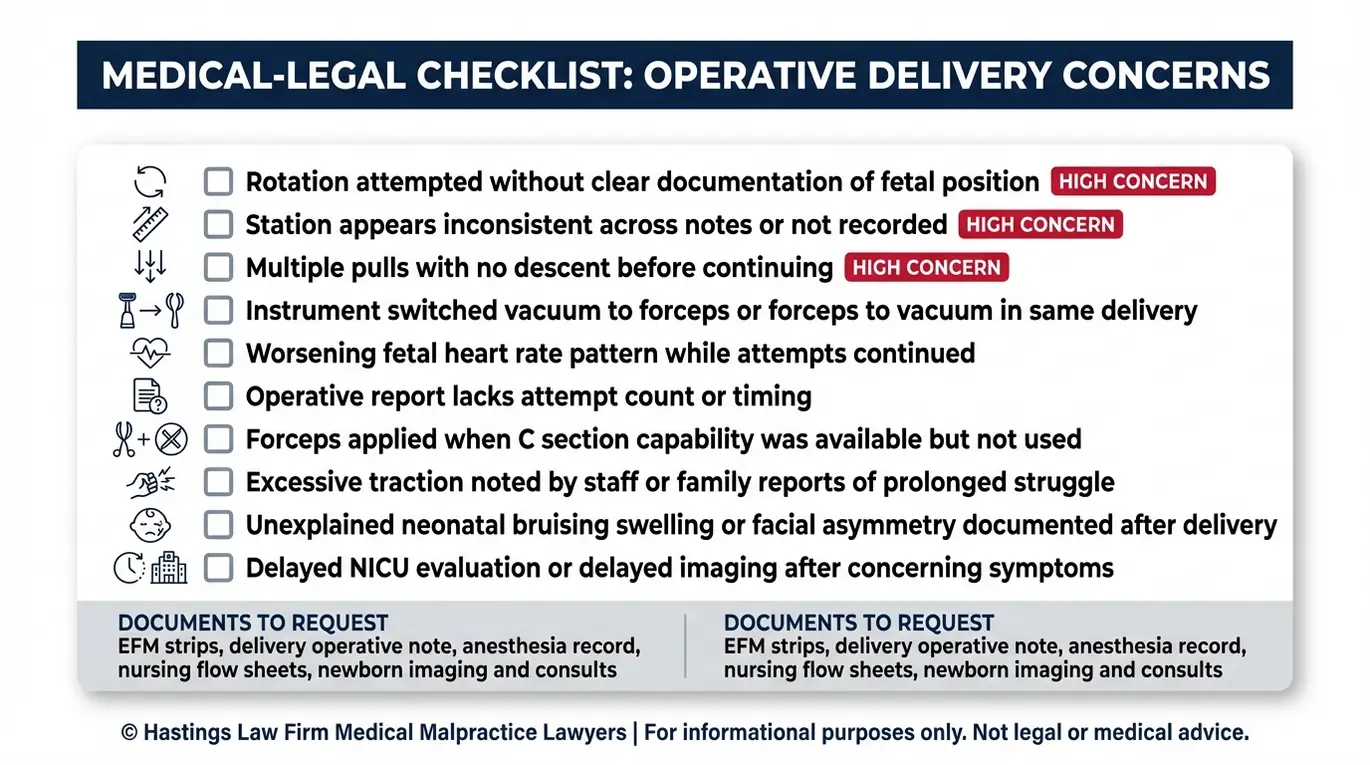
Red flags a rotational forceps negligence attorney may look for include:
- Forceps applied when fetal station was too high for the procedure
- Continued attempts after three or more unsuccessful pulls
- Use of both vacuum extraction and forceps in the same delivery
- Non-reassuring fetal heart rate patterns present before or during the procedure
- Inadequate documentation of fetal position and station in the medical records
- No documented informed consent discussion about the risks of operative vaginal delivery versus C-section
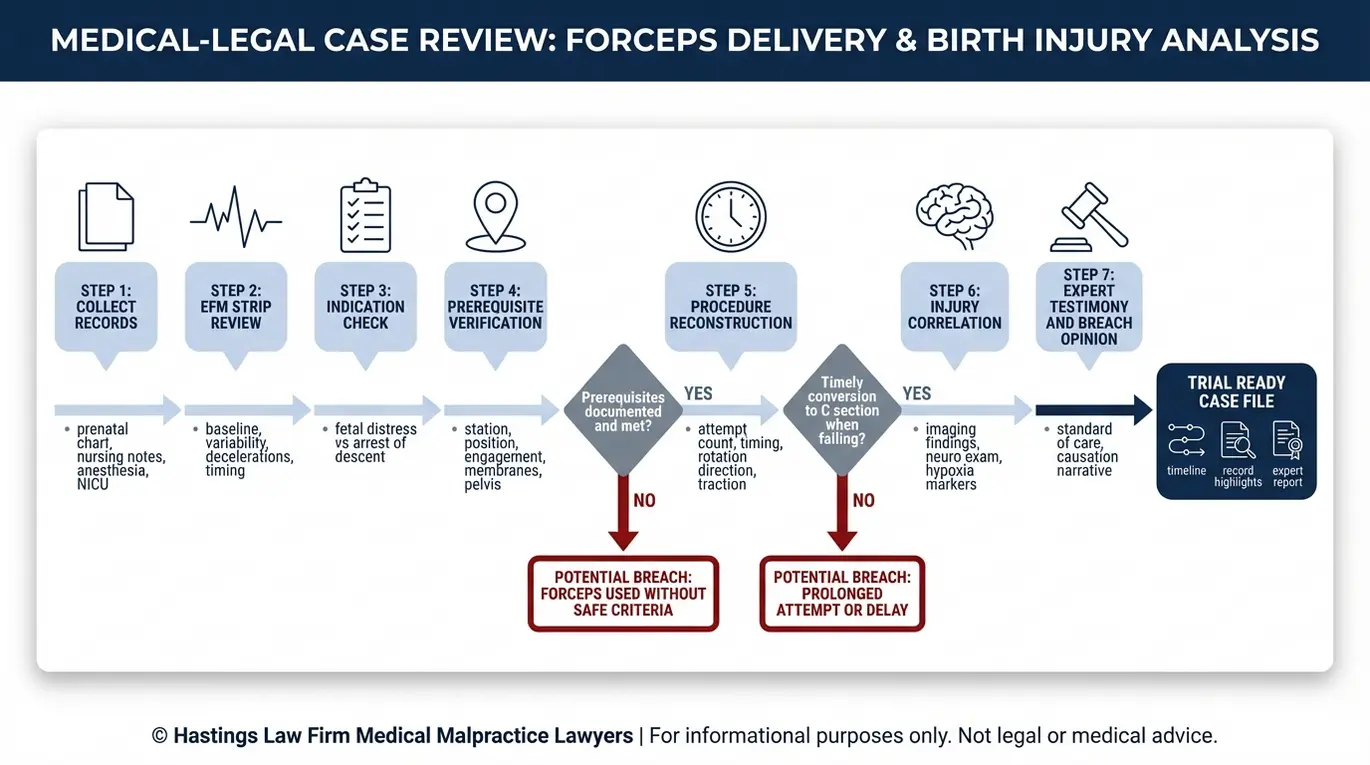
Proving Liability with Forensic Evidence
Proving liability requires a forensic analysis of the fetal heart rate strips, the delivery operative report, and expert testimony to establish that the physician violated the standard of care. We must use objective medical evidence to show exactly what went wrong. This is painstaking work, and it is where the medical and legal expertise of your legal team determines the strength of your case.
Step 1: Fetal Monitoring Strip Analysis
The electronic fetal monitor records the baby’s heart rate continuously during labor. Our Texas birth injury legal team begins by reviewing these strips minute by minute, looking for signs of fetal distress, such as late decelerations, variable decelerations, or prolonged bradycardia, that were present before the physician applied forceps. If distress was evident and the physician proceeded with an operative delivery instead of a C-section, that gap between what the data showed and what the doctor did becomes a central piece of the case. By correlating the heart rate tracings with the timing of the forceps application, we can demonstrate that the fetus was already compromised.
Step 2: Operative Report and Nursing Notes Review
The operative report is the physician’s own account of the delivery, including how they assessed fetal station and position, how many attempts were made, and the amount of traction applied. We compare this report against nursing notes, which are recorded in real time, to look for inconsistencies. Discrepancies between the doctor’s documented station assessment and the nurses’ charting can indicate that the clinical prerequisites for a safe forceps delivery were not actually met. We meticulously analyze these records to expose any attempts to retroactively justify a negligent procedure.
Step 3: Medical Records and Timeline Construction
We reconstruct a timeline of labor, from admission through delivery, using all available medical records. This timeline maps every decision point: when pitocin was administered, when the fetal heart rate changed, when the decision to use forceps was made, and how long each attempt lasted. Gaps or inconsistencies in this timeline often reveal where the standard of care broke down. For example, if the medical records show a delay between the onset of bradycardia and the delivery, we investigate what the medical team was doing during those critical minutes.
Step 4: Expert Testimony
Founded by Tommy Hastings, a board-certified trial lawyer, our firm maintains a national network of board-certified OB/GYN specialists who review medical evidence and provide testimony. Under Texas law, this expert analysis is not optional; it is required. Their testimony connects the evidence of hypoxia, improper technique, or ignored fetal distress signals to the child’s injuries.
Recovering Damages for Catastrophic Birth Injuries
Compensation may include coverage for lifelong medical care, loss of future earning capacity, pain and suffering, and specialized therapies required for the child’s development. Legal settlements are designed to provide financial security for an injured child. In cases involving permanent conditions like cerebral palsy or severe brain injury, the financial needs of the child can span decades.
Life Care Planning
A child with a catastrophic birth injury may require 40 to 60 years or more of ongoing medical care. These plans outline the medical and support services a child will need throughout their lifetime. This includes nursing support, adaptive equipment such as wheelchairs, occupational and physical therapy, surgeries, medications, and home modifications.
A birth injury lawyer works with life care planners and economists to project these costs accurately. Settlements must account for the full scope of the child’s future needs, not just current medical bills. Life care plans are dynamic documents that account for various stages of the child’s life, from pediatric care through adolescence and into adulthood. We review comparable verdicts to ensure that the demand we make on your behalf reflects the true cost of the injury.
Economic Damages
Economic damages cover the calculable financial losses caused by the injury. These damages account for the specific financial burdens placed on the family. Items covered typically include:
- Past and future medical expenses
- Rehabilitation and therapy costs
- Special education and developmental services
- Home health care and attendant care
- Loss of future earning capacity
- Adaptive equipment and home or vehicle modifications
Under Texas law, economic damages are generally uncapped, which means there is no statutory limit on the amount a jury can award for these categories. In catastrophic injury cases, economic damages often form the largest portion of the recovery. This ensures that even if the cost of medical inflation rises significantly over the child’s life, the funds will be available to provide high-quality care without burdening the family.
Non-Economic Damages and the Texas Cap
Non-economic damages address pain, suffering, physical impairment, and loss of enjoyment of life. Texas does place a damage cap on these awards under Chapter 74 of the Texas Civil Practice and Remedies Code. The cap is approximately $250,000 for all physicians and healthcare providers combined, with additional recovery available against healthcare institutions (up to $250,000 per institution, capped at $500,000 total for all institutions), for a combined maximum of roughly $750,000. While this cap limits the non-economic recovery, it does not restrict the economic damages that cover the actual cost of caring for a child with permanent injuries. Our goal is to maximize the economic portion of the claim to secure your child’s financial security.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
If your child was injured during a forceps delivery, you deserve answers about what happened and whether it could have been prevented. As a Texas rotational forceps birth injury lawyer, Hastings Law Firm brings together board-certified trial attorneys, in-house nurse consultants, and a national network of medical experts to investigate these cases with the depth and precision they require.
Our firm was built on a single mission: to restore trust for families who have been failed by the healthcare system and to hold negligent providers accountable. We handle these cases on a contingency fee basis, which means you pay no attorney fees or costs unless we secure a recovery for you.
Contact us today for a free, confidential case evaluation. Let us review the medical records, identify what went wrong, and explain your legal options.
Frequently Asked Questions About Rotational Forceps Birth Injury in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
