

Texas Postpartum Hemorrhage Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Postpartum hemorrhage is severe bleeding after childbirth that can escalate quickly when warning signs are missed or treatment is delayed. Some bleeding is normal after delivery, but uncontrolled blood loss can lead to shock, organ failure, emergency surgery, or fatal outcomes. Breakdowns can happen before delivery through missed risk planning, during labor through inaccurate blood loss assessment, or after discharge through inadequate instructions about abnormal bleeding. If you or a loved one were harmed or worse due to postpartum hemorrhage malpractice in Texas, contact Hastings Law Firm for a free, confidential case review.

Compassionate Texas Medical Attorneys for Excessive Bleeding After Birth Claims
What You Should Know About Excessive Bleeding After Birth Claims in Texas:
- Outcomes can become life threatening when postpartum hemorrhage is not recognized and treated promptly.
- Harm can follow missed planning for known hemorrhage risks during prenatal care.
- Delayed treatment can result when blood loss is underestimated using visual estimation instead of quantified measurement.
- Severe injury can include shock, organ failure, emergency hysterectomy, or death when escalation to transfusion or surgery is delayed.
- Safety after discharge can be compromised when patients are not clearly warned about signs of secondary postpartum hemorrhage.
- Liability can extend beyond the delivering physician to hospitals and staff when monitoring failures or system breakdowns occur.
- Options for recovery can be lost if Texas filing deadlines are missed.
- Compensation can include medical costs, lost wages, pain and suffering, and loss of reproductive ability after emergency hysterectomy.
- Recovery can be limited by Texas caps on non economic damages even when the injury is severe.
- Case outcomes can depend on what prenatal records, labor and delivery notes, vital sign logs, and operative reports show about recognition and response.

A Healthcare Focused Law Firm
Postpartum hemorrhage is one of the leading causes of maternal death in the United States, and in many cases, it is preventable. If you or someone you love suffered serious harm from uncontrolled bleeding after childbirth, you may be wondering whether the medical team responded the way they should have. That question deserves a clear, honest answer.
At Hastings Law Firm, we focus exclusively on medical malpractice. Our team includes in-house nurse consultants and former defense attorneys who know how to review labor and delivery records, identify where protocols broke down, and build cases grounded in medical evidence. As a Texas Postpartum Hemorrhage Lawyer, we understand both the medical science and the legal standard required to hold negligent providers accountable.
If something feels wrong about the care you received, contact us for a free, confidential case evaluation. We can review what happened and explain your options.
Understanding Postpartum Hemorrhage and Severe Blood Loss
Postpartum hemorrhage is a severe complication characterized by excessive bleeding of more than 1,000 milliliters after birth which can lead to shock or organ failure if not treated immediately. PPH remains a leading cause of maternal mortality worldwide, highlighting the urgent need for swift medical action.
Some bleeding after delivery is expected. Lochia, the normal vaginal discharge of blood and tissue following childbirth, gradually tapers off over several weeks. PPH is different. It involves rapid, heavy blood loss that does not slow on its own and requires immediate medical intervention.
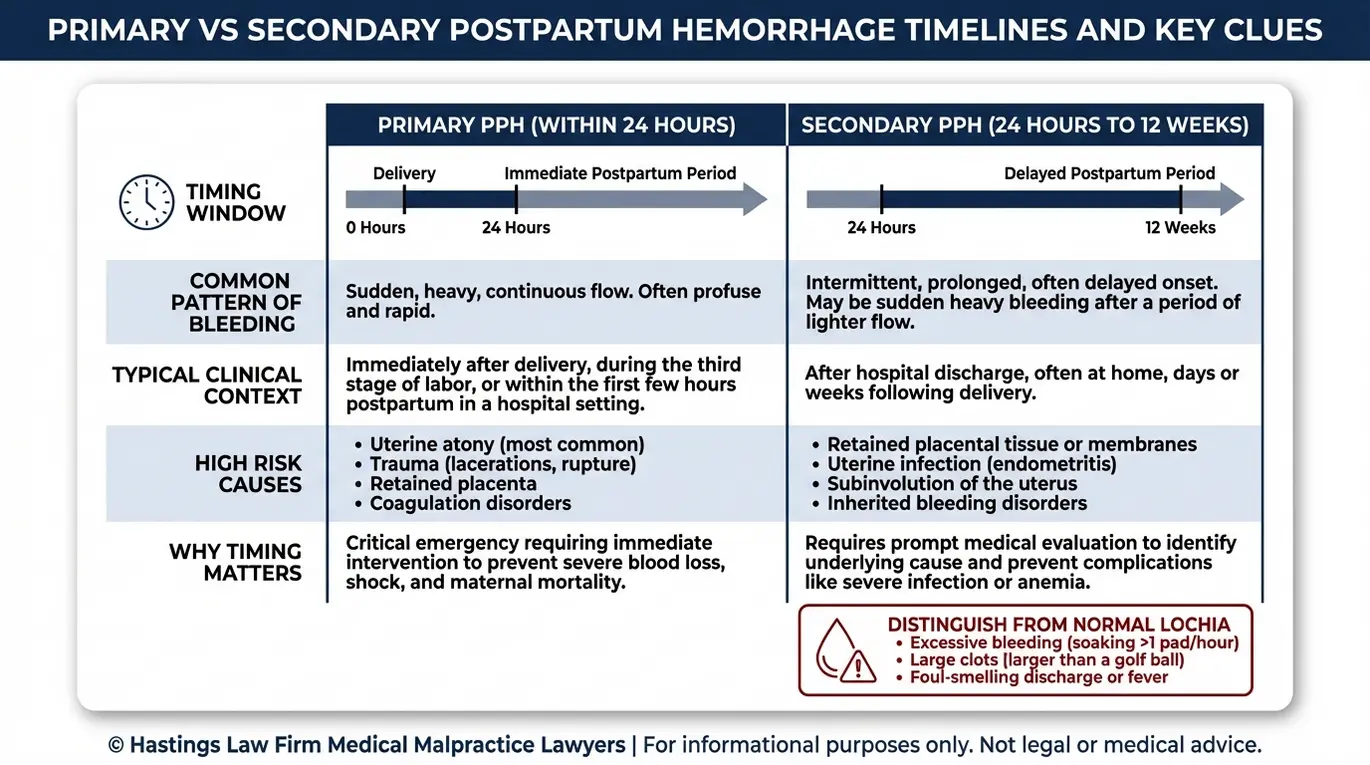
Timing matters both medically and legally. PPH is classified into two categories based on when the bleeding begins, and the distinction affects how the condition should be monitored and managed. This distinction is critical for determining whether the failure occurred during the hospital stay or due to inadequate discharge planning.
| Feature | Primary PPH | Secondary PPH |
|---|---|---|
| Onset | Within 24 hours of delivery | 24 hours to 12 weeks after delivery |
| Common Causes | Uterine atony, lacerations, retained placenta | Infection, retained placental tissue, subinvolution of the uterus |
| Detection Setting | Typically identified in the hospital | Often occurs after discharge |
| Key Risk | Rapid blood loss leading to hemorrhagic shock | Delayed recognition due to being home without monitoring |
Because secondary PPH can develop after a mother has already been sent home, proper discharge instructions and follow-up protocols are just as important as what happens in the delivery room. Patients must be educated on how to distinguish normal lochia from pathologic bleeding.
Rapid recognition is essential because the body’s compensatory mechanisms can only mask the signs of blood loss for so long before a sudden collapse occurs. When medical teams fail to respond quickly or miss the signs of hemorrhage entirely, the consequences can be devastating. Texas birth injury attorneys evaluate exactly these failures when building a case, looking for evidence that the provider missed the window to intervene before the situation became critical.
Common Causes and Risk Factors for Maternal Hemorrhage
The most common causes of postpartum hemorrhage follow the “4 Ts” mnemonic, which includes Tone (uterine atony), Trauma (lacerations), Tissue (retained placenta), and Thrombin (coagulation disorders). According to the National Center for Biotechnology Information (NCBI), these four categories account for the vast majority of PPH cases. Understanding these categories helps identify 4 Ts mnemonic errors that might have occurred.
Tone (Uterine Atony)
Uterine atony, meaning the uterus fails to contract firmly after delivery, is the single most common cause of postpartum hemorrhage. When the uterus does not tighten, the blood vessels at the former placental site continue to bleed freely. This condition is responsible for roughly 70 to 80 percent of all PPH cases.
Trauma (Lacerations and Injuries)
Physical injuries sustained during delivery can cause significant bleeding. These include cervical or vaginal lacerations, perineal tears, and injuries caused by the use of forceps or vacuum extractors. Uterine rupture or surgical injury during a C-section can also fall into this category.
Tissue (Retained Placenta or Membranes)
If fragments of the placenta or amniotic membranes remain inside the uterus after delivery, the uterus cannot fully contract. This often occurs in cases of placenta accreta, where the placenta attaches too deeply to the uterine wall. Finding retained placental tissue is vital because it prevents the natural clotting process and can trigger delayed hemorrhage.
Thrombin (Coagulation Disorders)
Pre-existing or pregnancy-related clotting disorders can impair the body’s ability to stop bleeding. Conditions such as HELLP syndrome, severe preeclampsia, or inherited coagulation deficiencies all increase the risk of hemorrhage that resists standard treatment.
Beyond the 4 Ts, several known risk factors raise the likelihood of PPH. These include prolonged labor, carrying multiples, preeclampsia, obesity, and a history of prior hemorrhage. When a patient presents with one or more of these factors, the medical team should be on heightened alert and prepared to act quickly.
We evaluate whether the care team identified these risks and responded appropriately based on the clinical picture.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Standard of Care for Preventing and Managing Hemorrhage
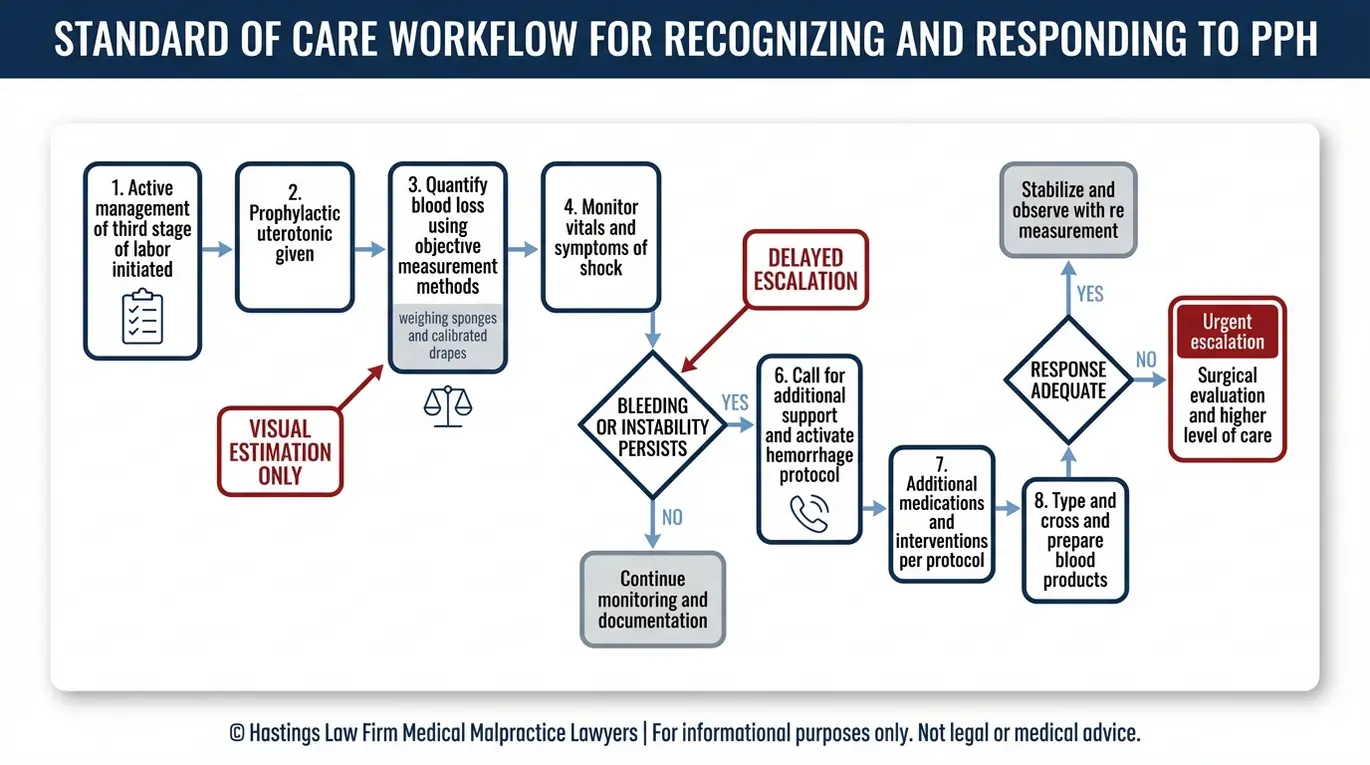
The standard of care requires medical providers to actively manage the third stage of labor, the period between delivery of the baby and delivery of the placenta, using uterotonics and to quantify blood loss accurately rather than relying on visual estimation. This standard defines the legal benchmark for what a competent medical team should do in a specific situation.
Active Management of the Third Stage of Labor (AMTSL) is the evidence-based protocol designed to reduce the risk of postpartum hemorrhage. It involves three core steps: administering a uterotonic medication (typically Oxytocin or Pitocin) immediately after delivery, applying controlled cord traction to help deliver the placenta, and performing uterine massage to encourage contraction.
Hospitals are also expected to use quantified blood loss (QBL), a measurement method that involves weighing surgical sponges and collecting fluids to calculate the actual volume of blood lost. Research published by Nursing CE Connection has shown that visual estimation of blood loss is dangerously inaccurate, often underestimating the true volume by 30 to 50 percent. When providers rely on visual estimation alone, they may not recognize a hemorrhage until the patient is already in distress.
Our team examines whether providers followed these protocols. Here is what the standard of care generally requires at each stage:
- Administer prophylactic Oxytocin/Pitocin immediately after delivery of the baby
- Perform controlled cord traction and inspect the placenta for completeness
- Begin uterine massage and monitor uterine tone
- Quantify blood loss using weighing methods rather than visual estimation
- Continuously monitor vital signs, including blood pressure and heart rate, for early signs of shock
- Escalate to second-line interventions if bleeding does not respond to initial treatment
- Activate a massive transfusion protocol or administer a blood transfusion if blood loss exceeds safe thresholds
Each of these steps creates a decision point. When a provider skips a step, delays escalation, or underestimates blood loss, the window for effective treatment narrows rapidly.
When Postpartum Hemorrhage Becomes Medical Malpractice
Medical malpractice occurs when a healthcare provider deviates from the standard of care by failing to diagnose hemorrhage risks or delaying necessary interventions like blood transfusions or surgery. Legal negligence occurs when a provider’s actions fall below established medical benchmarks.
One of the most common failures involves the prenatal period. If a patient has known risk factors, such as placenta accreta spectrum (PAS), a group of conditions where the placenta attaches too deeply into the uterine wall, the delivery team should plan accordingly. Failure to screen for or act on these conditions before labor begins can set the stage for a preventable crisis.
During labor and delivery, errors may include relying on visual estimation of blood loss rather than quantified measurement, delaying the administration of uterotonics, or failing to identify hemorrhage risks, resulting in misdiagnosis of the patient’s stability. Research from a clinical reconstruction study published in PubMed confirms that visual estimation consistently underestimates actual blood loss, which can cause a critical delay in treatment.
Surgical errors also give rise to malpractice claims. A nicked artery during a C-section or a delayed decision to perform an emergency hysterectomy when conservative measures are failing can result in catastrophic blood loss, organ damage, or death. In the most tragic scenarios, these failures lead to wrongful death.
Delayed-onset hemorrhage presents its own set of legal issues. When patients are discharged without proper warnings about the signs of secondary PPH, they may not seek care until the bleeding has already become dangerous. We review discharge instructions, follow-up scheduling, and nursing notes to determine whether the hospital met its obligations.
Under Texas Civil Practice and Remedies Code, Chapter 74, a medical malpractice claim requires proof that the provider’s conduct fell below the standard of care and directly caused the patient’s injury. As a Texas Postpartum Hemorrhage Lawyer, we work with qualified medical experts to reconstruct the timeline and identify exactly where the standard was breached. We build this case by comparing what happened against what should have happened at every decision point.
Identifying Liable Parties in Texas Birth Injury Cases
Liability in postpartum hemorrhage cases may extend beyond the delivering physician to include the hospital, nursing staff, or even the federal government, depending on where the injury occurred and who was responsible for the patient’s care. Liability depends on whether the provider is an employee or an independent contractor.
Private OB/GYNs often maintain hospital privileges but are not employees of the hospital. They typically carry their own malpractice insurance and are directly liable for errors they make during labor, delivery, and postpartum management. Since they are not employees, the hospital is generally not responsible for their independent medical judgments unless specific exceptions apply. If your obstetrician failed to respond to hemorrhage warning signs or made a surgical error, the claim may be directed at that physician individually.
Hospital Staff and the Institution bear separate responsibility. Nurses, anesthesiologists, and surgical technicians are typically hospital employees. When a nurse fails to accurately monitor blood loss or delays notifying the physician of declining vital signs, the hospital can be held liable for that employee’s negligence through a principle called vicarious liability. Hospitals may also face direct liability for systemic failures, such as inadequate staffing, missing equipment, or the absence of a hemorrhage protocol.
Our team includes former defense lawyers who previously represented the same hospital systems we now challenge. This background helps us understand how institutions evaluate these cases. We examine credentialing records, employment contracts, and staffing logs to determine which entities owed a duty of care and where that duty was breached.
Military and Federal Facilities present unique legal challenges. Texas is home to major military installations, including Fort Hood and Joint Base San Antonio. If the injury occurred at a military hospital or VA facility, the claim may fall under the Federal Tort Claims Act (FTCA), which imposes different filing requirements and deadlines than standard Texas malpractice claims.
These cases require an administrative claim with the appropriate federal agency before a lawsuit can be filed. These claims are complex because the government has sovereign immunity in many respects, meaning you must strictly adhere to the administrative exhaustion requirements of the FTCA before you can even step foot in a courtroom.
Compensation for Mothers Injured by Hemorrhage Negligence
Victims of postpartum hemorrhage negligence may recover compensation for medical bills, lost wages, pain and suffering, and in severe cases, the loss of reproductive ability due to emergency hysterectomy. Financial compensation helps families manage the long-term impact of a birth injury.
Economic damages cover the measurable financial costs. These include past and future medical costs, hospital stays, surgeries, rehabilitation, and any lost wages or reduced earning capacity resulting from the injury.
This Financial recovery is intended to restore the family to the financial position they would have been in had the negligence not occurred. In severe hemorrhage cases, the medical costs alone can be substantial, particularly when the patient requires extended ICU care or multiple blood transfusions.
Non-economic damages address the personal toll. Pain, suffering, mental anguish, and loss of enjoyment of life are all recognized categories of harm in Texas. The emotional impact of a birth injury can last a lifetime, affecting the mother’s relationship with her child and her overall mental health.
One of the most significant non-economic injuries in PPH cases involves emergency hysterectomy, the surgical removal of the uterus performed as a last resort to stop life-threatening bleeding. For a young mother, the permanent loss of reproductive ability carries profound emotional and psychological consequences that extend far beyond the operating room.
If postpartum hemorrhage results in a mother’s death, the family may pursue a wrongful death claim. These cases allow surviving spouses, children, and parents to seek compensation for loss of companionship, future financial support, and funeral expenses. We help identify the full scope of damages in your case, including future costs that may not be immediately obvious.
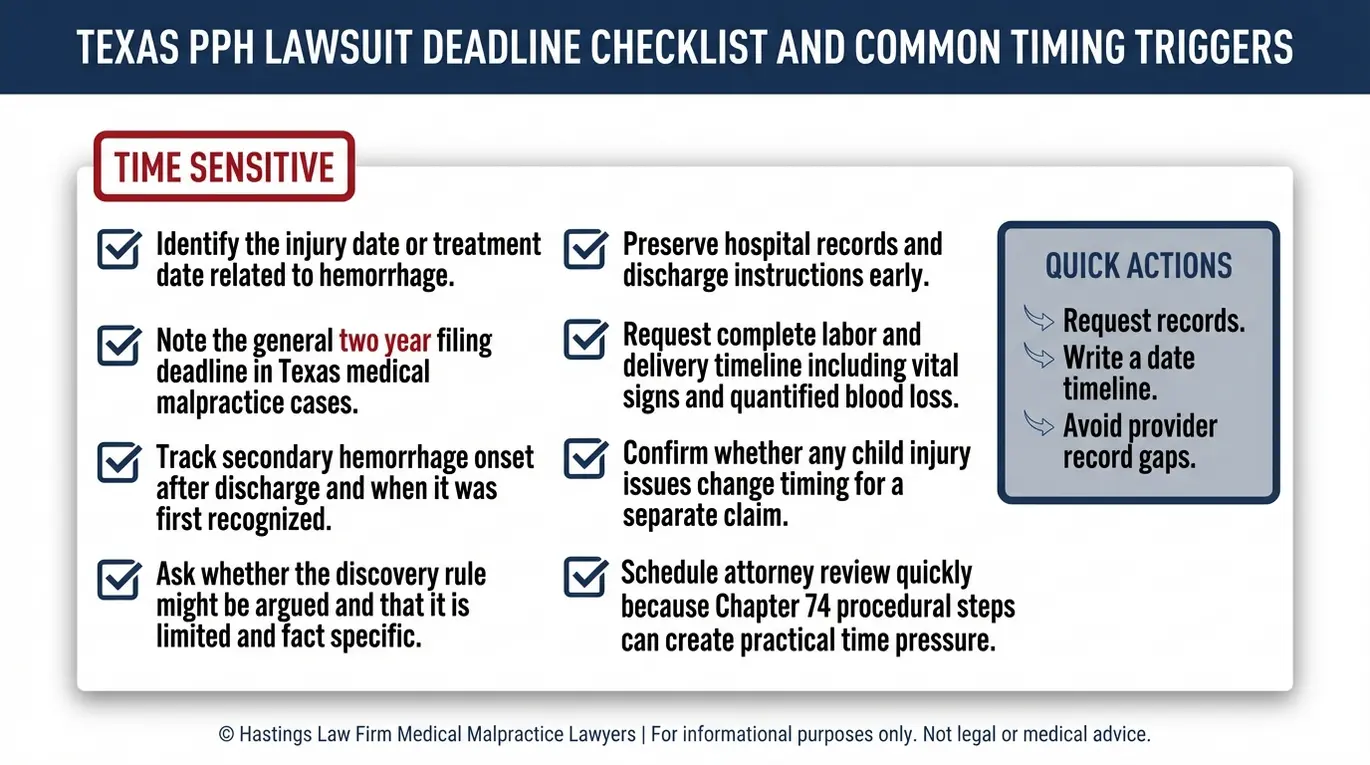
Texas Statute of Limitations for Postpartum Hemorrhage Lawsuits
In Texas, the statute of limitations for a medical malpractice claim is generally two years from the date of the injury, though exceptions may apply for cases involving delayed discovery or injuries to minor children.
This two-year deadline is established under Texas Civil Practice and Remedies Code, Chapter 74. Once the deadline passes, the court will almost certainly dismiss the case, regardless of how strong the evidence of negligence may be.
The Discovery Rule can be relevant in postpartum hemorrhage cases, particularly those involving secondary PPH. If the hemorrhage or its cause was not immediately apparent, such as when retained placental tissue triggers bleeding weeks after discharge, the two-year clock may begin on the date the injury was discovered or reasonably should have been discovered. However, Texas courts apply this exception narrowly, and it should not be relied upon without legal guidance.
Exceptions for Minors: If the child was also injured during the events that caused the mother’s hemorrhage, different tolling rules may apply to the child’s claim. The child’s statute of limitations may be extended, but the mother’s claim still operates under the standard adult deadline. Parents should not assume this tolling applies to their own claims, which remain subject to the standard two-year limit.
While the two-year statute of limitations is the primary deadline, Texas also enforces a ten-year statute of repose. This acts as an absolute bar to any claim filed more than ten years after the act of negligence, regardless of when the injury was discovered. Because these procedural rules are unforgiving, early legal consultation is essential to protect your rights.
⚠️ Do not wait to seek legal advice. Medical records can be altered, memories fade, and critical evidence becomes harder to obtain as time passes. Consulting a Texas medical malpractice lawyer early helps preserve the evidence needed to evaluate your claim and meet all filing deadlines.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
Postpartum hemorrhage is a known, treatable complication. When medical teams follow established protocols, most mothers recover safely. When they do not, the consequences can change a family’s life permanently.
If you or a loved one experienced serious harm from excessive bleeding after childbirth, Hastings Law Firm can help you understand what happened and whether negligence was involved. Our team of attorneys, nurse consultants, and medical experts reviews labor and delivery records with the clinical precision these cases require. Tommy Hastings, our founder, is board-certified in Personal Injury Trial Law and has over 20 years of experience in medical malpractice.
We operate on a contingency fee basis, which means you pay no attorney fees or costs unless we secure a recovery for you. Your initial consultation is free and confidential.
You deserve answers. Contact our Texas Postpartum Hemorrhage Lawyers today to schedule your risk-free case evaluation. Call us or fill out our online form to get started.
Frequently Asked Questions About Postpartum Hemorrhage in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
