

Texas Polyhydramnios Mismanagement Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Polyhydramnios is an excessive buildup of amniotic fluid that can raise the risk of serious complications when it is not identified, monitored, and managed appropriately. The text describes how diagnostic errors, missed trends in fluid levels, and delayed escalation of care can contribute to emergencies during pregnancy and delivery, including oxygen deprivation and permanent brain injury. It also discusses treatment options and medication risks, along with how disputes often focus on whether the response matched the severity of the condition. If you or a loved one were harmed or worse due to polyhydramnios mismanagement in Texas, contact Hastings Law Firm for a free, confidential case review.

Representing Texas Families Impacted by Preventable Birth Injuries
What You Should Know About Excessive Amniotic Fluid Birth Injury Claims in Texas:
- Catastrophic birth injuries can occur when excessive amniotic fluid is not properly managed, including oxygen deprivation that can lead to permanent brain injury or stillbirth.
- High risk delivery emergencies can become more likely when polyhydramnios causes uterine overdistension, including cord prolapse and placental abruption.
- Options for recovery in Texas can be limited for certain harms because non economic damages are capped while economic damages are not capped.
- Case outcomes can turn on whether providers recognized worsening fluid trends rather than relying on a single ultrasound reading.
- Harm can follow when elevated fluid levels are not met with increased surveillance such as serial ultrasounds and Doppler studies.
- Additional injury risk can arise when labor is induced in an overdistended uterus because the text links this to uterine rupture, placental abruption, and fetal distress.
- Medication related complications can become a central issue when indomethacin is used without careful monitoring because the text describes a risk to a fetal heart vessel.
- Legal options can be lost in Texas if required expert support is not provided on time because an expert report requirement acts as a gatekeeping measure.
- Key records can be central in disputes over timing and response, including fetal monitoring strips, ultrasound records, nursing notes, and provider orders.

A Healthcare Focused Law Firm
When your child suffers a birth injury that could have been prevented, the weight of that knowledge can be overwhelming. If your pregnancy involved polyhydramnios, or excessive amniotic fluid, and your medical team failed to manage the condition properly, you may have questions about what went wrong and what comes next.
At Hastings Law Firm, we focus exclusively on medical malpractice litigation. Our team includes in-house nurses, former defense attorneys, and board-certified trial lawyers who understand both the medicine and the law behind these cases. As a specialist in this field, Tommy Hastings is Board Certified in Personal Injury Trial Law by the Texas Board of Legal Specialization. Our team is prepared to review what happened during your care and help you understand your legal options.
If your family has been affected, we invite you to contact us for a free, confidential case evaluation. There is no fee unless we recover compensation on your behalf.
Understanding Polyhydramnios and the Risks of Excessive Amniotic Fluid
Polyhydramnios is a medical condition characterized by an excessive accumulation of amniotic fluid during pregnancy, which can increase the risk of severe birth complications if not properly identified and managed. While amniotic fluid cushions the baby, supports lung development, and maintains a stable temperature, too much of it can create serious risks for both mother and child.
According to the NCBI Bookshelf overview of Polyhydramnios, the condition affects roughly 1–2% of pregnancies. In some cases, the cause is unknown. In others, identifiable risk factors are present, and the standard of care requires that providers screen for and recognize them early.
Common risk factors associated with polyhydramnios include:
- Gestational diabetes, one of the most frequent causes of excess amniotic fluid
- Fetal anomalies, including gastrointestinal obstructions or neural tube defects that prevent the baby from swallowing fluid normally
- Twin-to-twin transfusion syndrome (TTTS), a dangerous condition in identical twin pregnancies where blood flow is unevenly shared between the twins through the placenta
- Fetal anemia, which can cause the baby’s body to increase urine output, raising fluid levels
When these risk factors are identified, the standard of care mandates a proactive approach. For instance, if gestational diabetes is the underlying cause, controlling maternal blood sugar levels becomes a primary strategy to manage fluid volume. Failure to address the root cause allows the fluid to continue accumulating, pushing the pregnancy from a manageable state into a high-risk category.
The distinction between mild and severe polyhydramnios matters significantly. Mild cases may only require increased monitoring. Severe cases demand aggressive management because the risks to mother and baby escalate quickly as the uterus struggles to contain the volume. Our medical malpractice lawyers help families determine whether providers responded appropriately to the severity of the condition, or whether critical warning signs were overlooked.
Diagnostic Errors and Failure to Monitor Amniotic Fluid Levels
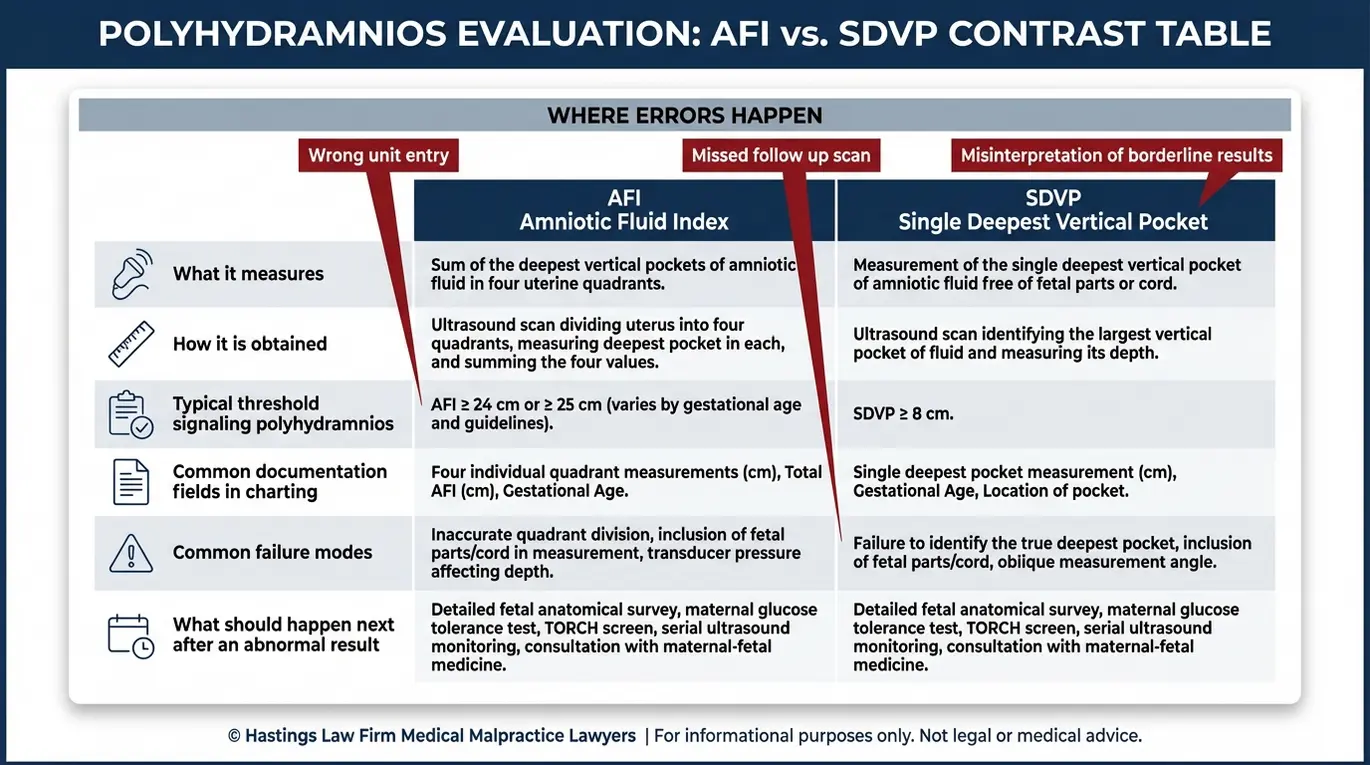
Doctors must diagnose polyhydramnios using ultrasound technology to measure the Amniotic Fluid Index (AFI) or Single Deepest Vertical Pocket (SDVP), with an AFI above 24 cm or an SDVP above 8 cm generally indicating a problem. Two primary methods are used: the AFI, which is calculated by dividing the uterus into four quadrants and adding the deepest fluid measurement from each, and the SDVP, also called the maximum vertical pocket (MVP), which measures the single deepest area of fluid.
The NCBI Bookshelf resource on Sonography Evaluation of Amniotic Fluid explains how these measurements guide clinical decision-making. Once elevated fluid levels are detected, the standard of care typically calls for increased surveillance, including serial ultrasounds and Doppler ultrasound studies to assess blood flow in the baby and placenta.
| Measurement Method | Normal Range | Polyhydramnios Threshold | What It Measures |
|---|---|---|---|
| Amniotic Fluid Index (AFI) | 5–24 cm | Greater than 24 cm | Sum of deepest pockets in four uterine quadrants |
| Single Deepest Vertical Pocket (SDVP/MVP) | 2–8 cm | Greater than 8 cm | Single deepest pocket of fluid |
Negligence in diagnosis can take several forms. A provider may fail to order follow-up ultrasounds after an initial abnormal reading. They may misinterpret the data, recording a measurement as borderline when it actually exceeds the threshold. Or they may fail to investigate the underlying cause of the elevated fluid levels.
Errors often occur when providers rely on a single, isolated measurement rather than looking at the trend of fluid accumulation over time. A borderline reading at 30 weeks that spikes significantly by 32 weeks represents a dynamic change that requires investigation, even if the absolute numbers are not yet catastrophic. Negligence may involve a failure to appreciate this trajectory, leading to a delay in referring the patient to a maternal-fetal medicine specialist for more advanced imaging. Our legal team will examine your medical records to determine whether the appropriate diagnostic steps were taken and whether any delays in identification contributed to harm.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Severe Complications Caused by Unmanaged Polyhydramnios
Unmanaged polyhydramnios causes dangerous uterine overdistension, a condition where the uterus is stretched beyond its normal capacity by the excess fluid. This overdistension significantly increases the risk of several life-threatening emergencies for both mother and baby during pregnancy and delivery.
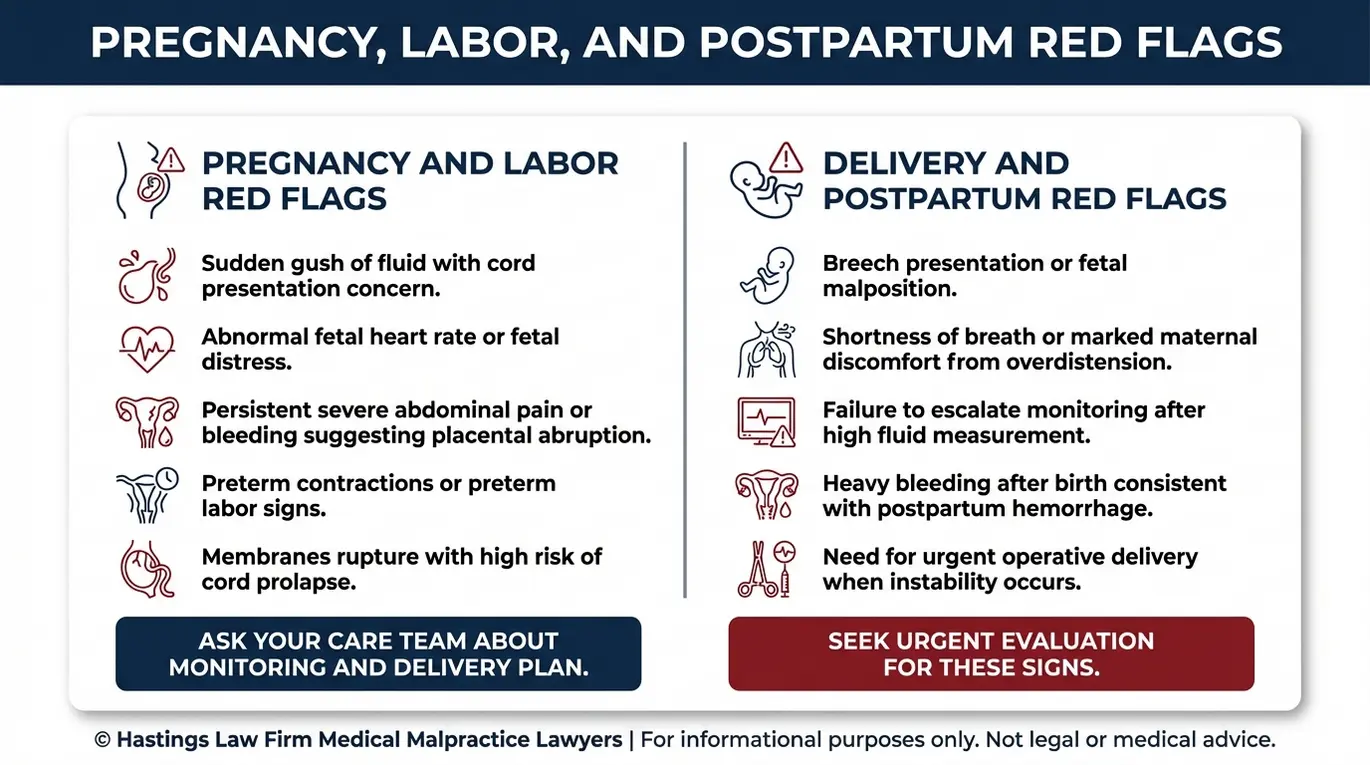
The mechanical pressure created by too much fluid weakens the uterine wall and destabilizes the baby’s position. That instability can trigger a cascade of complications, including:
- Preterm labor, which can begin when the overstretched uterus contracts prematurely under the strain of excess fluid. Because the uterus is a muscle, it reacts to extreme stretching by contracting, much like a rubber band that is pulled too tight. This reaction can trigger labor contractions well before the baby’s lungs are fully developed.
- Premature rupture of membranes (PROM), where the amniotic sac breaks early, potentially before the baby is mature enough for safe delivery. The membranes can only withstand a certain amount of tension before they rupture under the pressure.
- Breech presentation or fetal malposition, because the excess fluid gives the baby too much room to move, making it difficult for the baby to settle into a head-down position.
- Umbilical cord prolapse, a medical emergency where the umbilical cord slips through the cervix ahead of the baby, which can cut off the baby’s oxygen supply. The NCBI Bookshelf resource on Umbilical Cord Prolapse identifies polyhydramnios as a recognized risk factor for this complication.
- Placental abruption, where the placenta detaches from the uterine wall prematurely, causing severe bleeding and depriving the baby of oxygen and nutrients. When the uterus is overdistended, a sudden release of fluid, such as when waters break, can cause a rapid change in surface area. This rapid decompression can shear the placental abruption away from the uterine wall.
- Postpartum hemorrhage, excessive bleeding after delivery caused by the uterus being too stretched to contract effectively.
Intra-amniotic Pressure Risks
In symptomatic polyhydramnios, intra-amniotic pressure, the fluid pressure inside the uterus, rises to levels that can directly compromise fetal safety. Symptomatic cases involve maternal discomfort, respiratory difficulty, and visibly rapid uterine growth. The elevated pressure can restrict blood flow through the placenta and increase the likelihood of fetal distress.
When these symptoms are present, we evaluate whether the care team recognized the urgency and responded with appropriate interventions, or whether a failure to act allowed these preventable complications to develop.
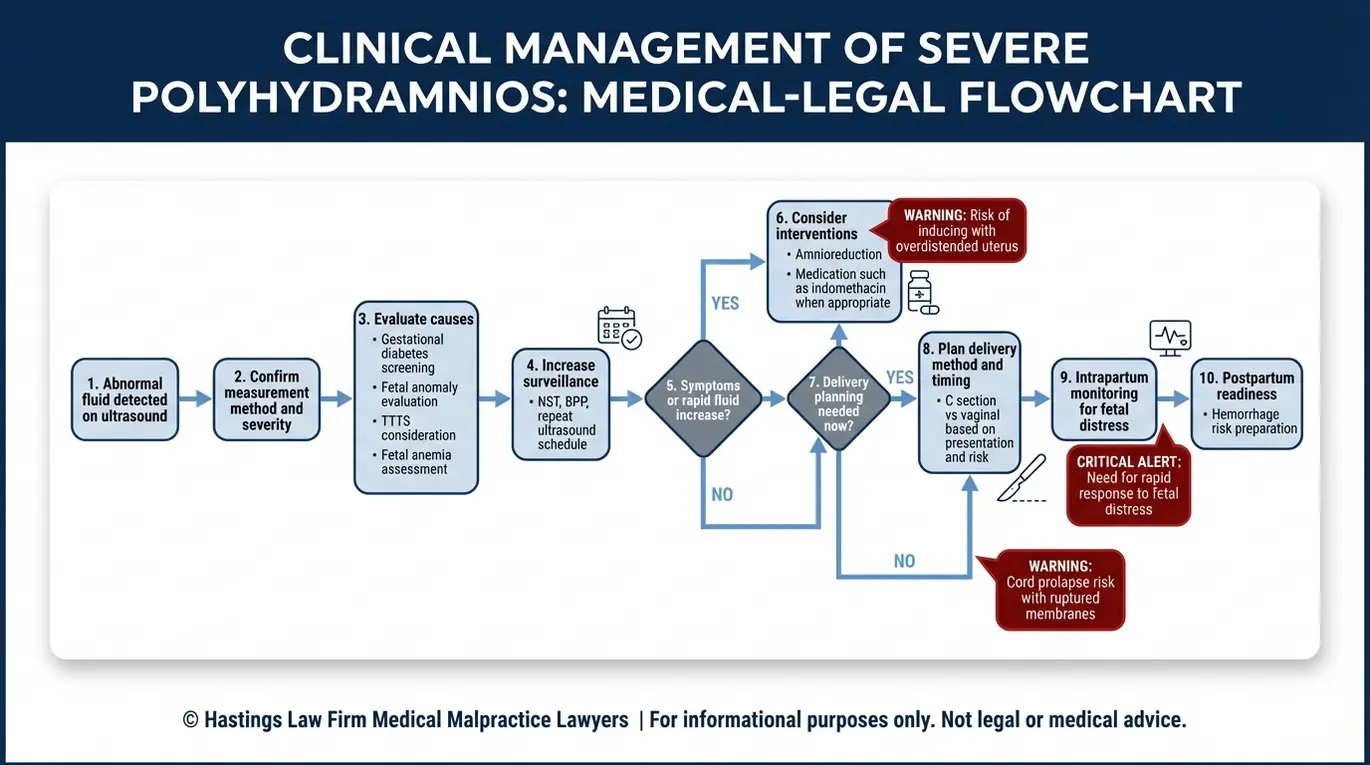
Proper Management Standards and Treatment Protocols
The standard of care for managing severe polyhydramnios may involve amnioreduction to drain excess fluid, medication to slow fluid production, or carefully planned delivery to avoid trauma to both mother and baby. The specific approach depends on gestational age, severity, and the underlying cause.
Recognized treatment options include:
- Amnioreduction, a procedure where a needle is inserted into the amniotic sac to drain excess fluid and reduce uterine pressure. This can be repeated as needed but carries its own risks, including infection and preterm labor.
- Indomethacin, a medication that reduces fetal urine output and can slow fluid accumulation. Providers must monitor its use carefully because of the risk it poses to the baby’s heart.
- Increased fetal surveillance, including Non-Stress Tests (NST) to track the baby’s heart rate patterns and Biophysical Profiles (BPP) to assess overall fetal well-being. A Biophysical Profile is a comprehensive exam that combines ultrasound findings with a non-stress test. It scores the baby on breathing movements, muscle tone, body movement, and amniotic fluid volume. A low score indicates that the baby is struggling in the intrauterine environment and may require immediate delivery.
- Planned delivery via C-section, particularly when the baby is in a breech position or when the risk of cord prolapse is high.
The University of Cincinnati’s clinical protocol on Isolated Amniotic Fluid Disorders outlines structured approaches that reflect current best practices for monitoring and intervention.
One area we examine closely in these cases is whether labor was induced using Pitocin when the uterus was already overdistended. Stimulating contractions in an overstretched uterus can increase the risk of uterine rupture, placental abruption, and fetal distress. Delivery timing and method require careful clinical judgment, and we review whether those decisions fell within the accepted standard of care.
Indomethacin and Drug Risks
Indomethacin, a nonsteroidal anti-inflammatory medication, is sometimes used off-label to reduce amniotic fluid levels. While it can be effective, its use carries a specific and well-documented risk: constriction of the ductus arteriosus, a blood vessel in the baby’s heart that must remain open during fetal development.
If this vessel narrows prematurely, it can cause serious cardiac complications for the baby. Providers must adhere to strict gestational age limits when prescribing this drug. Because of this risk, Indomethacin is generally avoided after 32 weeks of gestation. When providers prescribe it beyond that window or fail to monitor the baby’s heart with regular echocardiograms, it may represent a deviation from the standard of care.
Birth Injuries Resulting from Mismanaged Fluid Levels
Failure to manage high amniotic fluid levels can lead to catastrophic birth injuries, including Hypoxic-Ischemic Encephalopathy (HIE), a form of brain damage caused by oxygen deprivation during or shortly before delivery. HIE occurs when the baby’s brain does not receive enough oxygen for a sustained period, and it is one of the most devastating outcomes our team handles in polyhydramnios cases.
The chain of events often follows a recognizable pattern. Uterine overdistension from excess fluid can lead to placental dysfunction, cord compression, or abruption. Any of these can reduce or cut off the baby’s oxygen supply, resulting in hypoxia. If the medical team does not recognize the signs of fetal distress and act quickly, the Hypoxic-Ischemic Encephalopathy (HIE) can cause permanent brain injury.
The brain is highly sensitive to drops in oxygen levels. When hypoxia occurs, brain cells begin to die within minutes. In severe cases, this leads to multi-organ failure and necessitates therapeutic hypothermia (cooling) immediately after birth to limit the extent of the damage. However, even with advanced neonatal care, the damage done during those critical minutes of oxygen deprivation cannot always be reversed.
A systematic review published in PubMed Central examining the relationship between neonatal HIE and long-term cognitive outcomes confirms that even moderate HIE can result in lasting cognitive and developmental impairments. Children who survive severe HIE may face cerebral palsy, intellectual disabilities, seizure disorders, and a lifetime of medical care needs.
In the most tragic cases, prolonged oxygen deprivation leads to stillbirth. For parents, learning that their baby died in utero due to a condition that was known and monitorable is a devastating trauma. When a pregnancy has been identified as high-risk due to polyhydramnios and the medical team fails to intervene appropriately, the loss of a baby who could have been saved raises serious questions about the care that was provided.
Our team works with medical experts to reconstruct the timeline of events and determine whether earlier intervention could have prevented the outcome.
Proving Medical Malpractice in Polyhydramnios Cases
To prove malpractice, a plaintiff must demonstrate that the obstetrician deviated from the standard of care by failing to appropriately monitor fluid levels or intervene when signs of distress appeared, and that this failure directly caused the infant’s injury.
Under Texas law, medical malpractice claims require proof of four legal elements:
- Duty: The healthcare provider owed a duty of care to the patient. In obstetric cases, this duty exists from the moment the provider accepts the patient.
- Breach: The provider failed to meet the accepted standard of care. This could include failing to diagnose polyhydramnios, failing to increase monitoring, or choosing an inappropriate delivery method.
- Causation: The breach directly caused or substantially contributed to the injury. This is often the most contested element, requiring expert analysis to connect the provider’s actions (or inactions) to the harm.
- Damages: The patient or child suffered measurable harm, whether physical injury, the need for ongoing medical care, pain and suffering, or loss of future earning capacity.
Our team reconstructs a detailed medical timeline for every case. We review fetal monitoring strips, ultrasound records, nursing notes, and provider orders to identify exactly when the standard of care was breached.
Under Texas Civil Practice and Remedies Code Chapter 74, plaintiffs in medical liability cases must serve an expert report within 120 days after the defendant files an original answer. This report must be supported by a qualified medical professional who can speak to both the standard of care and causation.
This requirement is a gatekeeping measure in Texas law. The report must detail the physician’s qualifications, the specific standards that applied to the patient’s care, and exactly how the defendant’s departure from those standards resulted in the injury. Creating this report requires a meticulous analysis of the medical records by a retained expert witness before the case can even proceed fully.
This is why our trial-ready approach matters. When suing for polyhydramnios negligence, we prepare every case as though it will go before a jury, building a strong evidentiary foundation from day one. Our in-house medical staff and national network of expert witnesses allow us to identify breaches early, anticipate defense arguments, and negotiate from a position of strength. If you need a medical malpractice lawyer for amniotic fluid errors, our team has the clinical and legal experience to evaluate your standard of care thoroughly.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
If your child suffered a birth injury that you believe was connected to mismanaged polyhydramnios, you deserve answers. Our team at Hastings Law Firm is here to help you understand what happened and whether the care you received met the standard your family deserved.
Led by board-certified trial attorney Tommy Hastings, our firm brings together former defense lawyers, in-house nurses, and nationally recognized medical experts to build cases that hold negligent providers accountable. We believe that every family impacted by medical error deserves both the truth and a path toward financial security for their child’s future.
We handle these cases on a contingency fee basis, which means you pay no attorney fees or costs unless we recover compensation for your family.
Contact a Texas polyhydramnios mismanagement lawyer at Hastings Law Firm today for a free, confidential case evaluation. Let us review your medical records and explain your options.
Frequently Asked Questions About Polyhydramnios Mismanagement in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
