

Texas Nursing Home Medication Error Lawyer
Written by: Hastings Law Firm | Reviewed by: Gabe Sassin | Updated: July 27, 2026
Medication errors in nursing homes are often preventable and can cause serious harm in residents who are older or medically fragile. Problems like wrong doses, missed medications, identity mix ups, and dangerous drug interactions are frequently tied to understaffing, poor training, and breakdowns during transfers. Records such as the Medication Administration Record can help show what was ordered and what was actually given. If you or a loved one were harmed or worse due to nursing home medication negligence in Texas, contact Hastings Law Firm for a free, confidential case review.

Compassionate Texas Medical Attorneys for Nursing Home Medication Negligence Claims
What You Should Know About Nursing Home Drug Error Claims in Texas:
- Severe harm or fatal outcomes can follow nursing home medication errors because residents are often medically fragile.
- Accountability can extend beyond a single nurse when facility systems like staffing, training, and medication controls contribute to repeated errors.
- Harm can occur during transitions of care when medication lists are not updated correctly after a hospital return.
- Life threatening overdoses can result when extended release medications are crushed for feeding tube administration and the full dose absorbs at once.
- Recovery options can be limited if early procedural requirements are missed, since Texas law can allow dismissal for noncompliance.
- Financial recovery can be constrained because Texas caps non economic damages in medical malpractice cases.
- Compensation can include economic losses like medical expenses and non economic losses like pain, suffering, and loss of independence.
- Wrongful death claims may be available when a medication error causes a resident to die.
- Case clarity can depend on whether MAR and eMAR records match physician orders and pharmacy inventory logs.
- Disputes can arise when documentation shows late entries, backdated charting, or repeated identical notes across shifts.

A Healthcare Focused Law Firm
When someone you love is harmed by a preventable medication error in a nursing home, the experience can feel deeply personal and deeply unfair. You trusted a facility to provide safe, attentive care, and that trust was broken. The confusion that follows is normal. So is the frustration of not knowing exactly what went wrong or who is responsible.
A Texas nursing home medication error lawyer can help you find those answers. At Hastings Law Firm, our team focuses exclusively on medical malpractice. Our founder, Tommy Hastings, is Board Certified in Personal Injury Trial Law by the Texas Board of Legal Specialization.
We understand how medication errors happen in long-term care settings, and we know how to investigate them. If your family member was harmed by a drug error in a Texas nursing facility, we can review what happened. We explain your legal options at no cost and with no obligation.
Common Types of Medication Errors in Texas Nursing Homes
Medication errors in nursing homes typically involve administering the wrong drug, wrong dose, or wrong form to a resident, often resulting from systemic failures rather than isolated accidents. Because nursing home residents tend to be older and medically fragile, even a seemingly minor error can lead to serious harm or death.
A nursing home drug error attorney sees certain patterns come up again and again. Wrong dosage errors, for example, may involve giving too much of a sedative or too little of an important pain medication. Opioids require precise measurement, and even a slight miscalculation can suppress breathing. Similarly, insulin dosages must change based on real-time blood sugar readings; failing to adjust the dose can lead to hypoglycemic shock, or dangerously low blood sugar.
In other cases, a resident receives a drug intended for someone else entirely due to an identity mix-up during medication rounds. In chaotic environments, staff may rely on memory rather than checking wristbands or photos. This leads to mix-ups where a resident receives a cocktail of medications meant for a neighbor with different medical needs.
Omission errors are also common. A resident who depends on insulin for blood sugar control may miss a scheduled dose, triggering a dangerous metabolic event. Equally concerning are adverse drug interactions that occur when staff fail to check whether a new prescription is contraindicated, meaning it should not be combined with another drug the resident is already taking.
This risk is especially high in residents on multiple medications, a situation known as polypharmacy. Drugs like anticoagulants (blood thinners such as warfarin), opioids, and sedatives carry elevated risks when combined improperly or administered without proper monitoring.
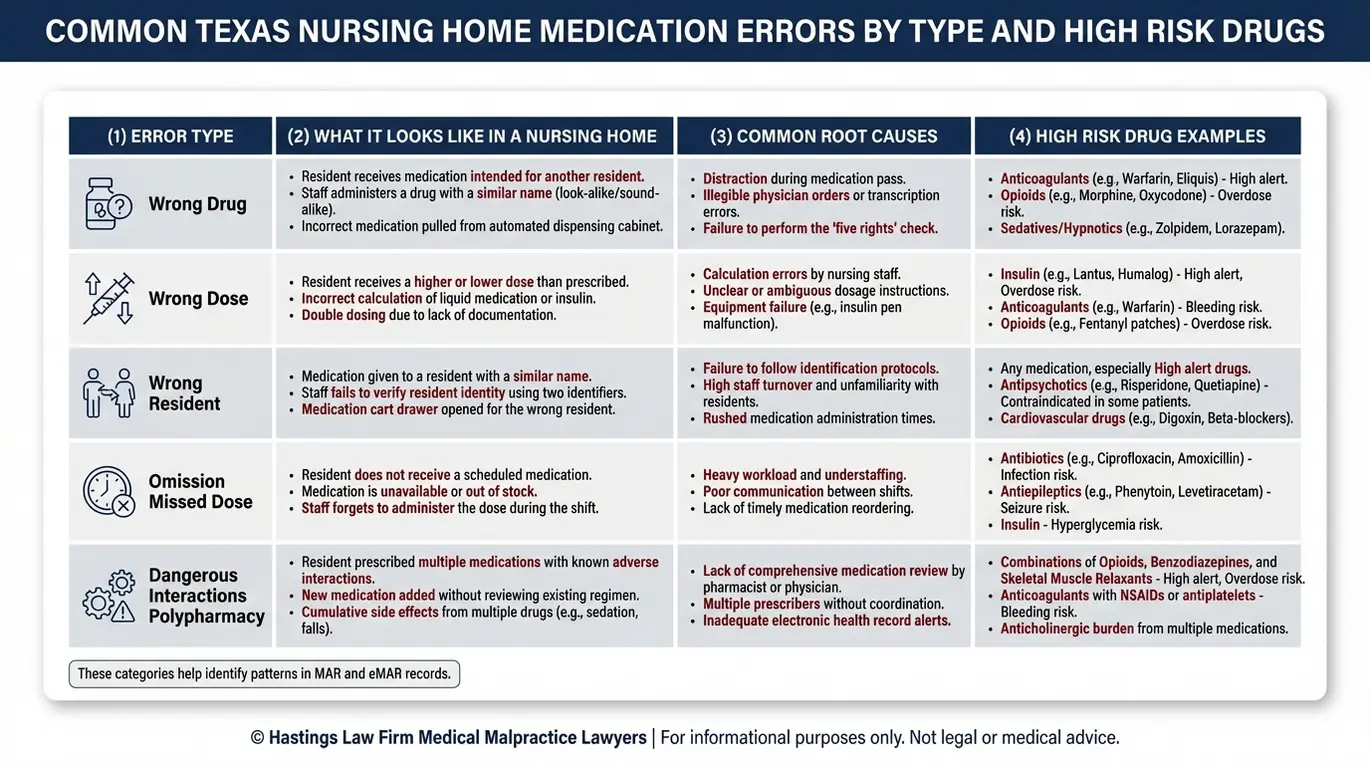
A medication negligence lawyer evaluates these situations by examining what protocols were in place, whether they were followed, and where the breakdown occurred. The table below summarizes the most common categories we encounter:
| Error Type | Common Examples | High-Risk Drugs |
|---|---|---|
| Wrong Dosage | Overdose of sedatives; underdose of pain medication | Opioids, Sedatives, Insulin |
| Wrong Patient | Medication given to incorrect resident during rounds | Any scheduled medication |
| Omission | Missed or skipped doses of essential medication | Insulin, Warfarin, Cardiac drugs |
| Adverse Interactions | Contraindicated drugs prescribed together without review | Anticoagulants, Opioids, Sedatives |
Each of these categories represents a preventable failure. When a facility’s own systems allow these errors to happen repeatedly, the problem is not just individual carelessness. It points to deeper institutional breakdowns in how medications are ordered, stored, verified, and administered.
Why Do Drug Errors Happen in Long-Term Care Facilities
Most medication errors stem from chronic understaffing, inadequate training, and communication breakdowns during shift changes or patient transfers. These are not random events. They are predictable consequences of nursing home neglect and systemic problems that facility management has a responsibility to address.
A nursing home negligence lawyer knows that when a nursing home does not employ enough qualified staff, nurses and aides are often rushed through medication rounds. CMS regulations set federal standards for nursing home quality and staffing. Failure to adhere to these regulations often means nurses are rushed, making it far more likely that someone will skip important safety steps.
The clinical standard for safe medication administration is built around the 5 Rights of Medication Administration, a framework that requires verifying the right patient, right drug, right dose, right route, and right time before giving any medication. When staff members are stretched too thin, one or more of these checks gets bypassed.
Training deficiencies compound the problem. Staff may lack adequate knowledge about specific drug protocols. They may not understand that certain extended-release pills should never be crushed, or that a particular combination of medications requires closer monitoring. Poor facility-level protocols for ordering, stocking, and tracking medications add another layer of risk.
Common root causes of medication errors in long-term care include:
- Understaffing: Too few nurses covering too many residents, leading to skipped safety checks
- Inadequate training: Staff unfamiliar with specific drug handling requirements or interaction risks
- Poor communication: Incomplete handoffs between shifts or transfer reconciliation
- Systemic protocol failures: Lack of standardized procedures for verifying and documenting medication orders
- Polypharmacy management gaps: No reliable system for reviewing residents on multiple prescriptions, a condition called polypharmacy, where the risk of harmful drug interactions increases with every additional medication
As a medication error attorney, we examine these institutional factors carefully. Individual staff mistakes matter, but they almost always trace back to a system that made the error possible.
Dangerous Administration via Feeding Tubes
One particularly dangerous category of error involves residents who receive nutrition and medication through an enteral feeding tube, such as a PEG tube (placed directly into the stomach) or an NG tube (passed through the nose). Enteral feeding tubes provide nutrition and medication directly to the stomach or through the nose. Proper care for these tubes is necessary to prevent severe complications.
When oral medications must be given through a feeding tube, staff sometimes crush pills that were specifically designed not to be crushed. Extended-release medications, often labeled ER or XR, are formulated to dissolve slowly over many hours. Crushing these pills destroys that controlled-release mechanism and drastically alters the intended absorption rate, causing the full dose to absorb at once.
This phenomenon is called “dose dumping.” Dose dumping occurs when a full dose of medication is released into the body all at once, which can lead to life-threatening overdoses. Proper training and clear facility protocols should prevent this from ever happening. When it does, it reflects a serious lapse in the standard of care.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Cognitive Failures and Transfer Reconciliation Issues
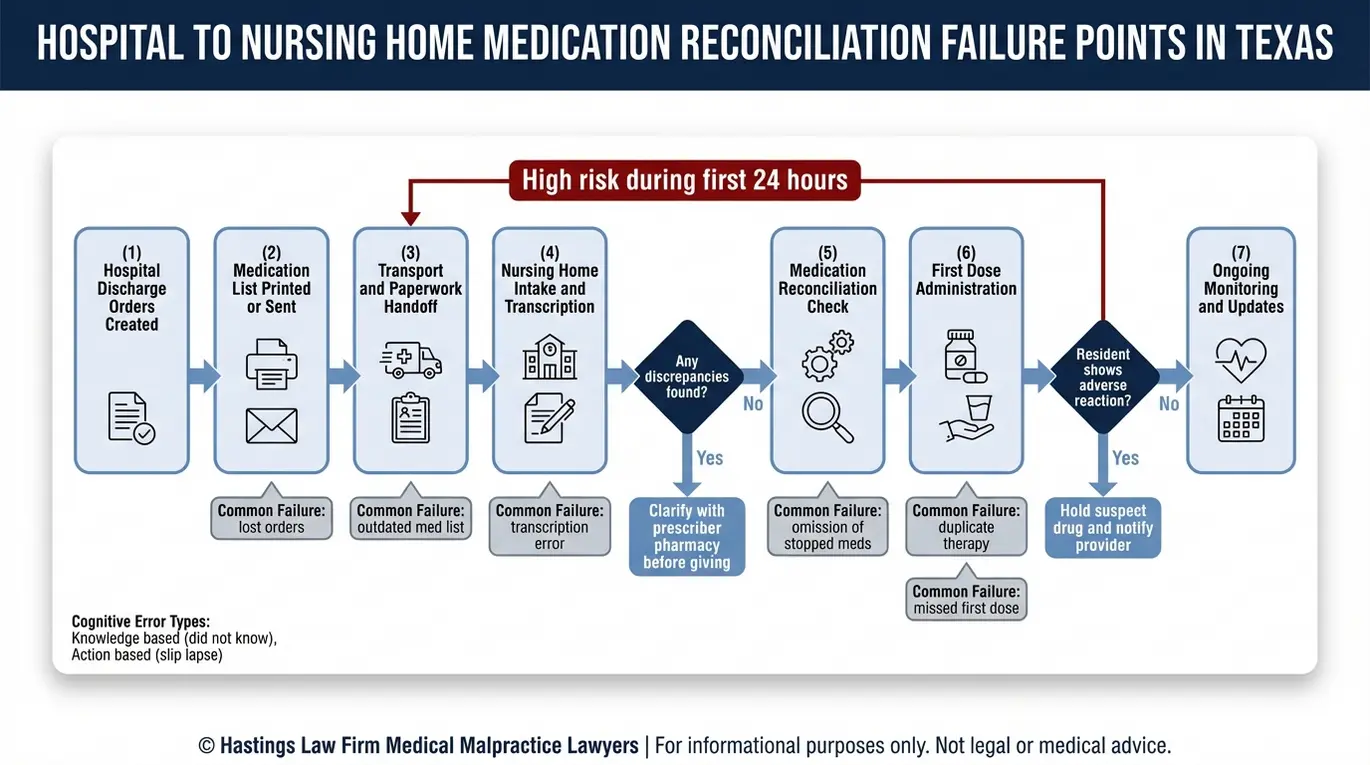
Errors frequently occur during “handoffs,” such as when a resident returns from a hospital, leading to reconciliation failures where medication lists are not updated correctly. These transition points are among the highest-risk moments in a nursing home resident’s care.
The hospital-to-nursing-home transfer is a critical point where orders get lost or transcribed incorrectly. A hospital physician may discontinue one drug and start another, but if that change is not recorded correctly, the resident may end up taking both or neither. Medication reconciliation is the process of comparing a resident’s current list against new orders to catch conflicts, omissions, or duplications.
According to the Centers for Medicare and Medicaid Services (CMS), this reconciliation step is a required quality measure. Yet it remains one of the most common points of failure, leading to reconciliation errors.
These errors are not simply random accidents. Researchers categorize these mistakes to distinguish between errors based on lack of knowledge and errors based on physical actions. A nurse may intend to grab the correct medication but, due to distraction or fatigue, inadvertently selects a look-alike pill from the cart. These slips are symptoms of an environment that lacks adequate safeguards.
Both types are preventable with proper systems, training, and oversight. As a Texas nursing home lawyer, we evaluate the transfer documentation, intake records, and pharmacy logs to determine where reconciliation broke down and who bears responsibility.
A medical malpractice attorney experienced in these cases understands that the root cause often lies in the system itself, not just the individual who made the final mistake. We trace the full chain of communication to identify every point where a drug-drug interaction, which is a harmful reaction between two or more substances, or dosage conflict should have been caught.
Proving Negligence Using the Medication Administration Record
To prove negligence, attorneys must audit the Medication Administration Record (MAR) and eMAR to find discrepancies between the physician’s orders and what was actually documented as administered to the resident.
Attorneys focus on the Medication Administration Record (MAR), which is the core clinical document that tracks every dose of every medication a resident is supposed to receive. The eMAR audit trail is its electronic counterpart and provides a digital timeline of care. This log shows when entries were made, by whom, and whether any changes occurred after the fact. For a nursing home malpractice lawyer, these records are often the most important evidence in the case.
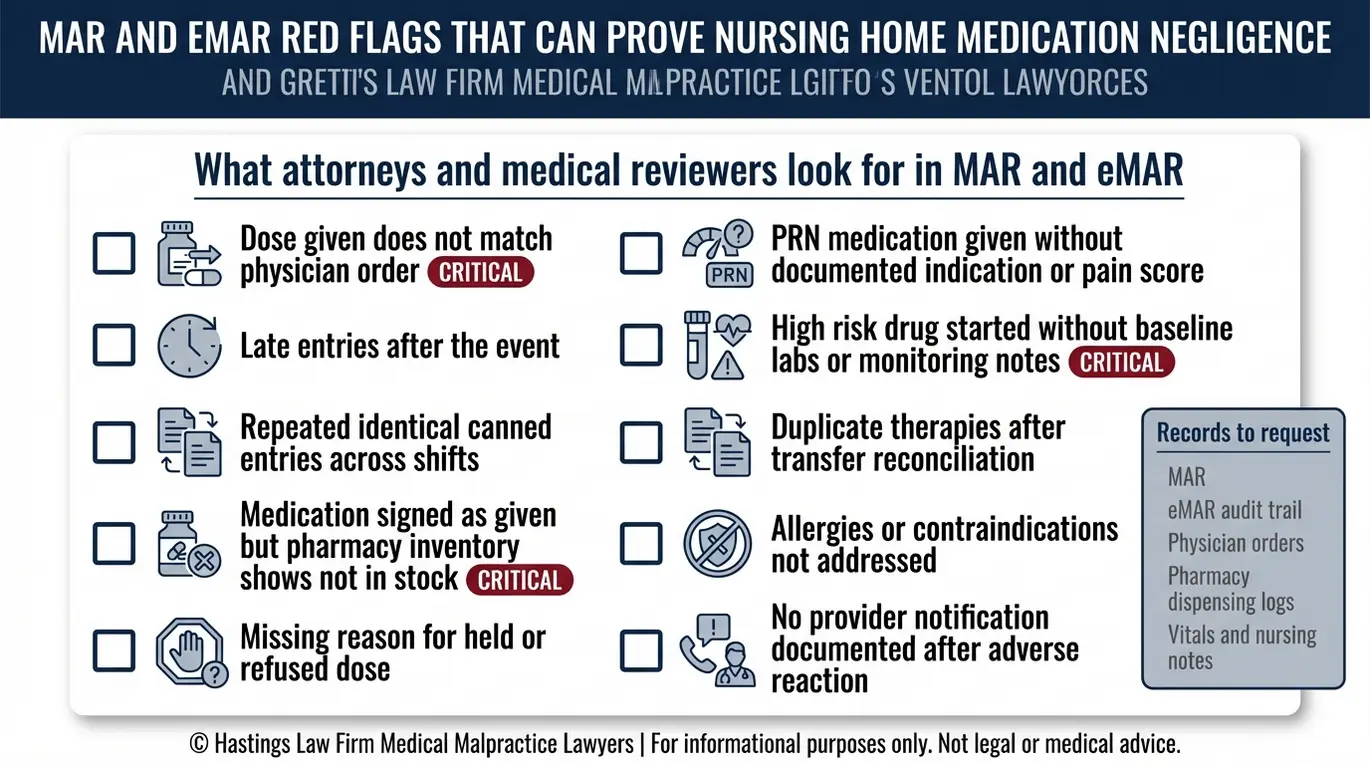
Our team includes experienced hospital nurses who previously worked for the systems they now challenge. Our in-house nurse consultants and medical staff review these records line by line, looking for specific red flags. The eMAR audit trail can reveal patterns that a surface-level review would miss, including late entries, backdated charting, or copy-pasted notes.
We also cross-reference the MAR against pharmacy inventory records. If a nurse signed off confirming a medication was given, but that medication was not in stock at the facility on that date, the documentation itself becomes evidence of a potential cover-up or systemic failure.
When reviewing a MAR, our team specifically looks for:
- Gaps where scheduled medications have no corresponding administration entry
- Late or backdated entries suggesting after-the-fact documentation
- Repeated identical notes across different shifts or different residents
- Discrepancies between physician orders and recorded doses
- Missing signatures or initials from administering staff
- Entries that conflict with pharmacy delivery and inventory logs
Texas law adds an additional procedural requirement that a medication injury attorney must address early. Under Texas Civil Practice and Remedies Code Chapter 74.051, a claimant must serve an expert report within 120 days of filing a healthcare liability claim.
This report, prepared by a qualified medical expert, must identify the applicable standard of care, explain how it was breached, and connect that breach to the resident’s injury. Our national network of medical experts allows us to meet this requirement with credible, well-supported testimony. Failure to file this report correctly can lead to the case being dismissed.
Who Is Liable for a Medication Error in Texas
Liability may extend beyond the nurse to include the nursing facility for negligent hiring, the attending physician for improper prescribing, or the pharmacy for dispensing errors.
The facility bears liability for its own institutional decisions. These include staffing levels, training programs, supervision protocols, and the systems used to manage medication administration. If a facility’s policies were inadequate or if facility management failed to correct known problems, the facility can be held directly responsible.
Vicarious liability, the legal principle that an employer can be held responsible for the negligent acts of its employees, may also apply when a staff member’s error occurred within the scope of their duties. Our team includes former defense attorneys who understand the internal systems of these facilities, which helps us identify where these institutional failures occur.
The prescribing physician may be liable if the medication order itself was improper. This includes prescribing a contraindicated drug, ordering an incorrect dosage, or failing to account for the resident’s other medications and known allergies. A Texas medical malpractice lawyer will review the prescribing records and consult with medical experts to evaluate whether the physician’s orders met the standard of care.
The pharmacy also has a role. If a pharmacist filled a prescription incorrectly, failed to flag a dangerous drug interaction, or dispensed the wrong medication or strength, the pharmacy may carry independent liability. We investigate every link in the chain to identify all responsible parties whose combined failures led to the injury.
Compensation and Damages for Medication Injuries
Victims of medication errors may recover economic damages for medical bills and non-economic damages for pain, suffering, and physical impairment, subject to Texas statutory caps. Texas law allows patients to seek financial recovery for injuries caused by medical negligence.
Economic damages cover the measurable financial losses caused by the error. These include:
- Past and future medical expenses required to treat the injury
- Costs for ongoing rehabilitation, therapy, or specialized care
- The expense of a Life care plan if the injury requires long-term assistance
A life care plan is particularly important for residents who survive a catastrophic error, such as hypoxic brain injury (brain damage from lack of oxygen) from an overdose. This detailed projection accounts for 24-hour nursing needs, specialized equipment, and home modifications for the remainder of the resident’s life.
Non-economic damages compensate for losses that do not carry a specific dollar amount but are no less real:
- Physical pain and suffering
- Mental anguish and emotional distress
- Loss of enjoyment of life and loss of independence
Under Texas Civil Practice and Remedies Code Chapter 74, non-economic damages in medical malpractice cases are capped. The general limit is $250,000 per institution, with total non-economic damages across all defendants typically capped between $500,000 and $750,000 depending on the number and types of defendants involved.
If a medication error caused a resident’s death, such as a morphine overdose or a fatal adverse reaction, the family may pursue a wrongful death claim. Wrongful death compensation can include loss of companionship, mental anguish of surviving family members, and funeral and burial costs. Nursing home injury compensation cases require careful documentation, and our team works with medical and financial experts to present a full picture of the harm.
Contact the Texas Nursing Home Attorneys at Hastings Law Firm Today for Help
If you believe your loved one was harmed by a medication error in a Texas nursing home, you do not have to figure this out alone. These cases involve complex medical records and institutional systems designed to protect the facility, not the resident. Our team, which includes former defense attorneys, in-house nurses, and patient advocates, knows how to uncover what happened.
Hastings Law Firm handles nursing home medication error cases on a contingency fee basis, which means you pay no attorney fees or costs unless we recover compensation for your family. As a Texas nursing home medication error lawyer, we prepare every case as though it is going to trial, because that preparation is what drives results.
Contact us for a free, confidential case evaluation. Let us help you find the answers you deserve and take the first step toward understanding your legal options.
Frequently Asked Questions About Nursing Home Medication Error in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Gabe Sassin has focused exclusively on medical malpractice law since 2007. After spending more than a decade as a malpractice defense attorney, he knows exactly how the other side works. He has seen firsthand how healthcare providers, insurers, corporate defendants, and their legal teams think, prepare, and build their defense against claims. That knowledge works for the people who need it most today, injured patients and their families. His unique experience shapes everything he writes, giving readers a look at how these cases actually work from someone who has handled them from both sides.
