

Texas NICU IV Extravasation Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
NICU IV extravasation injuries can leave families shocked and searching for clear answers about what went wrong. When an IV leaks into surrounding tissue, a newborn can suffer serious damage that may worsen quickly without prompt recognition and action. These events often involve missed warning signs, gaps in monitoring, or problems with catheter placement and securement, especially when vesicant medications are used. Understanding how extravasation happens and what records may show can help families make informed decisions. If you or a loved one were harmed or worse due to NICU IV extravasation in Texas, contact Hastings Law Firm for a free, confidential case review.

Advocating for Texas Families of Infants Injured by IV Errors
What You Should Know About Infant IV Insertion Error Claims in Texas:
- Permanent injury risk can rise quickly when NICU IV extravasation is not recognized and treated promptly.
- Severe tissue damage can occur when vesicant medications leak outside the vein, including chemical burns and tissue destruction.
- Disputes about preventability often focus on whether the IV site was monitored consistently and whether the infusion was stopped when warning signs appeared.
- Long term complications can include necrosis, scarring, nerve damage, compartment syndrome, and amputation in severe cases.
- Liability can extend to a hospital for employed staff actions under vicarious liability.
- Options for recovery in Texas can be limited by strict malpractice requirements and a cap on non economic damages.
- Compensation may include medical expenses for future care and surgery, as well as pain and suffering, disfigurement, and physical impairment.
- Documentation gaps can become central when electronic records and nursing logs do not show timely IV site assessments.
- Infusion pump data and medication records can be critical when the injury involves high risk vesicants.
- Photos and medical chart entries can be important for showing injury progression and the timing of clinical response.

A Healthcare Focused Law Firm
Discovering that your newborn was harmed during NICU care is deeply unsettling, especially when the injury may have been preventable. If your infant suffered tissue damage from an IV that leaked or was improperly monitored, you are not alone, and you have every right to ask questions about what happened.
At Hastings Law Firm, our team has focused exclusively on medical malpractice litigation since 2005, emphasizing cases where newborns are harmed by hospital errors. Our team of attorneys, in-house nurse consultants, and medical experts understands both the clinical and legal details that these cases demand. As Texas NICU IV extravasation lawyers, we are prepared to review your child’s medical records, identify what went wrong, and explain your legal options.
If your family is facing this situation, we invite you to contact us for a free, confidential case evaluation. There is no fee unless we recover compensation for your child.
Understanding IV Extravasation in the NICU
IV extravasation occurs when a catheter dislodges or leaks, allowing medication to escape into the surrounding tissue rather than the vein. In the NICU, this is especially dangerous because infants have fragile veins, thin skin, and no ability to tell anyone something hurts.
To understand these injuries, it helps to know the difference between two related but distinct events: IV infiltration and IV extravasation.
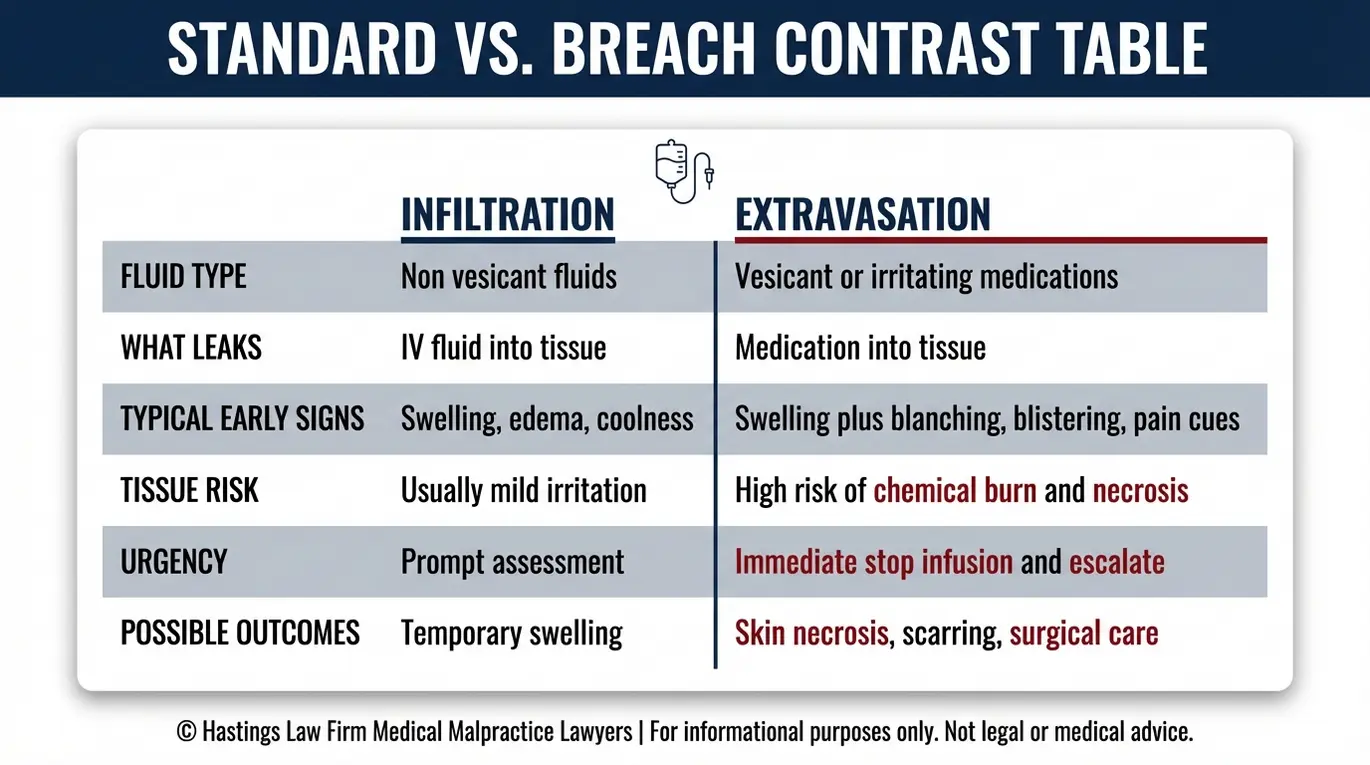
IV infiltration, a condition where a non-vesicant fluid leaks from the vein into nearby tissue, can cause swelling and discomfort but often resolves without lasting harm. IV extravasation, the leakage of a vesicant medication capable of causing chemical burns and destroying tissue on contact, is far more severe. The consequences of extravasation can be devastating if not treated immediately.
According to St. Jude Children’s Research Hospital, both conditions require prompt attention, but extravasation carries a much higher risk of permanent injury.
| Feature | IV Infiltration | IV Extravasation |
|---|---|---|
| Fluid type | Non-vesicant (saline, certain antibiotics) | Vesicant (caustic drugs that blister tissue) |
| Tissue response | Localized swelling, mild discomfort | Chemical burns, blistering, tissue death |
| Typical outcome if caught early | Resolves with elevation and observation | May still cause significant tissue damage |
| Typical outcome if missed | Temporary swelling or minor injury | Necrosis, scarring, potential limb loss |
Premature and critically ill newborns face elevated risk because their veins are extremely small and their skin is thinner than that of older children. A cannula, the thin tube inserted into the vein, can shift with even minor movement.
Because the ratio of the catheter size to the tiny vein is often high, blood flow can be easily obstructed. This increases back pressure and the chance of leakage. Since these infants cannot report pain or pull away in a way that alerts staff, the responsibility to catch problems early falls entirely on the nursing team.
When a Texas NICU malpractice attorney investigates these cases, the first question is almost always the same: how quickly did the care team recognize what was happening, and what did they do about it?
Signs of Extravasation in Non-Verbal Infants
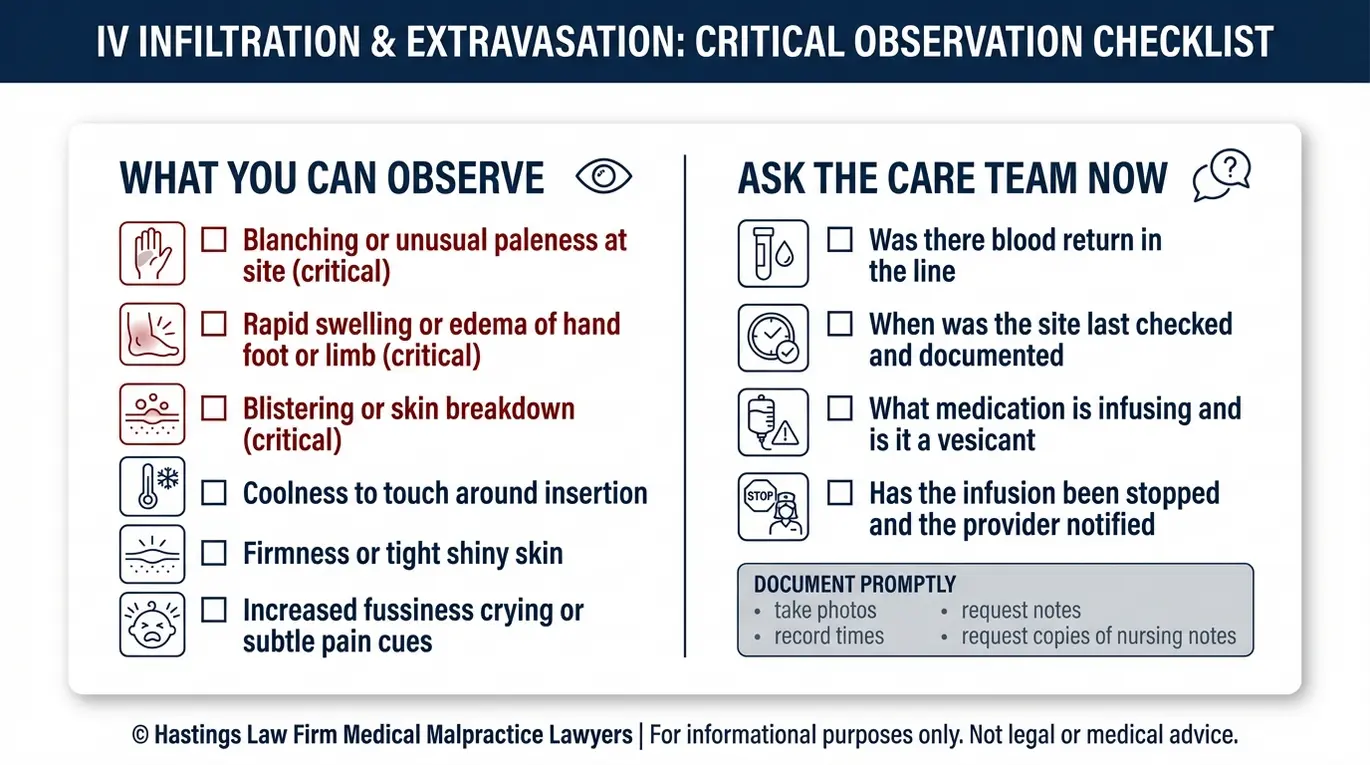
Since NICU patients cannot speak, nurses must rely on objective signs to detect IV complications. These include blanching, or paleness around the IV site, coolness to the touch, blistering, distinct swelling known as edema, or a lack of blood return when aspirating the line. These symptoms indicate a medical event where IV fluids or medications have migrated into the tissue space.
What Parents and Nurses Should Watch For
There are several observable warning signs, and parents who are present at the bedside may notice them before or alongside the nursing staff:
- Skin color changes: Discoloration, redness, or a dusky or mottled appearance near the IV site
- Swelling or firmness: The area around the insertion site becomes puffy, tight, or hard compared to the opposite limb
- Temperature changes: The skin near the IV feels noticeably cooler or warmer than the surrounding area
- Blistering or skin breakdown: Any visible blisters, peeling, skin necrosis, or open areas near the catheter
- Behavioral cues: Unexplained crying, changes in heart rate or oxygen levels, or visible distress during infusion
These signs can develop gradually, which is why consistent monitoring is so important. Research published in PubMed Central on peripheral venous extravasation injury confirms that early detection directly affects outcomes and that a failure to monitor properly is a leading contributor to severe tissue damage.
If you noticed any of these signs during your child’s NICU stay, or if you observed a change in your baby’s limb that was not addressed promptly, an infant IV injury lawyer can help you determine whether monitoring protocols were followed.
IV Staging Scale and Severity
Medical professionals use a standardized IV staging scale, a grading system to classify the severity of infiltration and extravasation injuries. This grading system is the clinical standard used to measure the depth and extent of the injury, typically graded from Stage 0 to Stage 4:
- Stage 0: No symptoms present
- Stage 1: Slight skin blanching, mild edema, skin cool to touch
- Stage 2: Moderate blanching, edema extending slightly beyond the IV site
- Stage 3: Significant blanching, edema spreading well past the site, possible numbness
- Stage 4: Deep tissue involvement, skin breakdown, necrosis, or tissue death, often requiring surgical intervention such as skin grafting
The higher the stage, the more likely the injury is to cause permanent harm. When we review a case, the documented stage at the time the extravasation was first noted, and how long elapsed before it was caught, can be critical evidence.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Common Causes of NICU IV Injuries
Most NICU IV injuries result from improper catheter placement, failure to secure the line, or—most critically—failure to monitor the site hourly according to standard nursing protocols.
Here are the most common breakdowns we look for when evaluating these cases:
- Insertion errors: Puncturing through the vein wall during the initial IV insertion, causing immediate leakage into tissue
- Catheter dislodgement: Failure to properly secure the peripheral IV cannula, the small, flexible tube placed in the vein, in an infant who may move unpredictably
- Monitoring gaps: The standard of care typically requires NICU IV sites to be assessed at least every hour; missed checks allow injuries to progress undetected
- Shift-change failures: Poor communication during nursing hand-offs about the condition or timing of the IV site assessment
When nurses change shifts, the hand-off process is a critical moment for patient safety. If the outgoing nurse fails to report the exact status of the IV line or the last time it was flushed, the incoming nurse may assume the line is functional without performing an immediate check, allowing an infiltration to continue for hours.
According to the University of Iowa Health Care’s clinical guide on pediatric IV infiltration and extravasation, early recognition and immediate intervention are essential to preventing serious tissue injury in neonatal patients.
As Texas NICU IV extravasation lawyers, we examine nursing logs, electronic medical records, and infusion pump data to build a minute-by-minute timeline. This timeline often reveals whether monitoring was performed as required or whether gaps in documentation suggest the IV site went unchecked for extended periods.
High-Risk Medications (Vesicants) in Neonatal Care
Certain medications, known as vesicants, cause severe chemical burns if they leak outside the vein. In neonatal care, these include calcium gluconate, potassium chloride, dextrose concentrations above 10%, and certain antibiotics like vancomycin.
A vesicant, any drug that can blister and destroy tissue on contact, poses significant danger to infants. A non-vesicant, a fluid that may cause swelling or irritation but does not typically result in tissue destruction, carries less risk.
Because the margin for error is so small with these drugs, hospitals often have specific “vesicant protocols” that require two nurses to verify the line placement before starting the infusion and more frequent checks during administration.
| Medication | Type | Risk If Extravasated |
|---|---|---|
| Calcium gluconate | Vesicant | Skin necrosis, deep tissue calcification |
| Potassium chloride | Vesicant | Chemical burn, tissue death |
| Dextrose (>10%) | Vesicant | Skin sloughing, necrosis |
| Vancomycin | Vesicant | Blistering, localized tissue damage |
| Normal saline | Non-vesicant | Swelling, typically self-resolving |
According to the NCBI Bookshelf’s reference table on vesicants and their antidotes, specific antidotes and interventions exist for many of these agents, but they must be administered quickly to be effective.
Our legal team includes former hospital nurses and former defense attorneys who previously worked for the systems they now challenge, providing us with internal insight into hospital protocols. A Texas birth injury attorney evaluates whether the clinical team followed these heightened protocols or whether the response was delayed.
Long-Term Complications: Necrosis and Scarring
Untreated extravasation can lead to full-thickness tissue necrosis requiring skin grafts, permanent nerve damage, compartment syndrome, and in severe cases, amputation of the affected limb or digits.
The progression of injury often begins with swelling that, left unaddressed, worsens into tissue death. Necrosis, the death of skin and underlying tissue, can develop within hours if the leaked medication continues to contact unprotected cells. Once tissue has died, it cannot recover on its own.
In many cases, surgical intervention becomes necessary. A fasciotomy, a procedure in which a surgeon cuts open the tissue layer to relieve dangerous pressure buildup, may be required. This can prevent compartment syndrome, a condition where swelling within a confined muscle space becomes so severe that it compresses nerves and vessels, risking permanent functional loss.
The DIVE2 study published in PubMed Central documented the range of injuries seen in pediatric extravasation cases, including scarring, disfigurement, and loss of movement that persists into childhood and beyond.
For a growing child, these injuries affect more than appearance. Nerve damage in the hand or foot can limit dexterity, grip strength, and mobility for years, sometimes permanently. When we work as Texas NICU IV extravasation lawyers for a family in this situation, the full scope of the child’s future needs, including reconstructive surgery, physical therapy, and adaptive care, becomes central to the case.
Proving Negligence and Hospital Liability
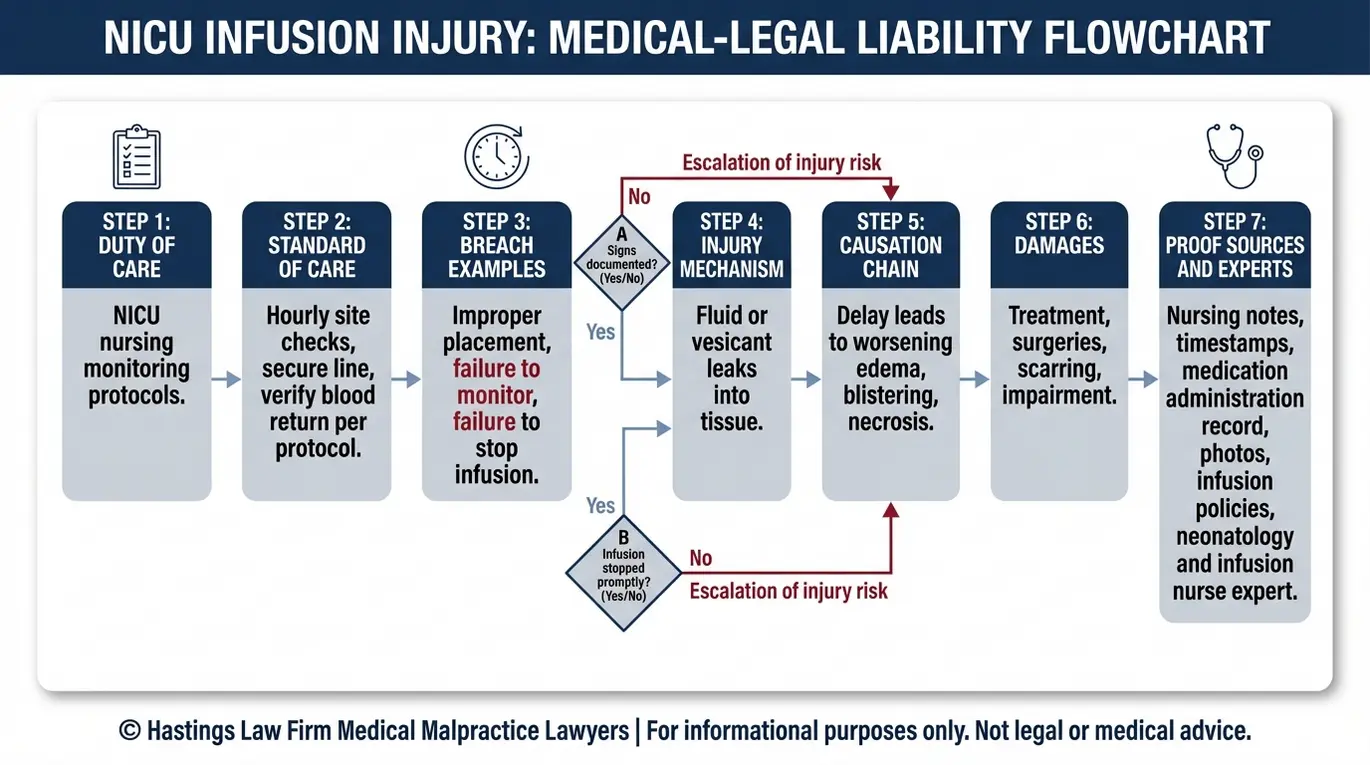
Establishing liability requires proving that the nursing staff deviated from the standard of care, typically by failing to assess the IV site frequently enough or failing to stop the infusion immediately when signs of injury appeared.
In Texas, medical malpractice claims require four elements: a duty of care owed to the patient, a breach of that duty, a causal connection between the breach and the injury, and resulting damages. These four elements form the legal framework for proving that a healthcare provider’s actions directly caused harm.
Here is how those elements apply in a NICU IV extravasation case:
- Duty: The NICU nursing staff has a duty to monitor IV sites at established intervals and respond to changes in the infant’s condition.
- Breach: A breach may occur if the nurse failed to check the site hourly, did not document assessments, or continued an infusion despite visible signs of extravasation. Electronic medical records often reveal these breaches by showing gaps in charted vitals or IV site assessments.
- Causation: We work with expert witnesses, including neonatologists and certified infusion nurses, to establish that earlier intervention would have prevented or reduced the severity of the injury.
- Damages: The resulting harm must be documented, from the initial tissue damage through any surgeries, scarring, or functional limitations.
Texas law also recognizes vicarious liability, meaning the hospital can be held accountable for the negligence of its employed nurses and staff. Our investigation typically includes a review of hospital staffing levels, training records, and internal protocols to determine whether systemic failures contributed to the injury.
Under Texas Civil Practice and Remedies Code Chapter 74, a qualified expert must provide a written report supporting the claim. As Texas medical malpractice lawyers, we work with nationally recognized medical experts who can explain how the standard of care was violated and how that violation caused your child’s injuries.
Damages and Compensation for Injured Infants
Compensation in Texas NICU cases may cover past and future medical expenses (including reconstructive surgery), pain and suffering, disfigurement, and physical impairment.
Texas law divides recoverable damages into two categories:
Economic damages are the tangible, calculable costs associated with the injury. These are not subject to a cap and may include:
- Emergency medical treatment and hospitalizations
- Reconstructive surgeries and skin grafting procedures
- Ongoing physical and occupational therapy
- Future medical care, adaptive equipment, and specialist visits
- Any other out-of-pocket costs directly related to the injury
Because a child’s life expectancy is long, these future costs must be projected over decades, often requiring a life care planner to estimate the total financial impact adjusted for inflation.
Non-economic damages compensate for harm that cannot be easily measured in dollars, including:
- Physical pain and suffering
- Mental anguish experienced by the child and family
- Disfigurement and scarring
- Loss of physical function or impairment
Texas does impose a statutory cap on non-economic damages in medical malpractice cases. Economic damages, which often represent the largest portion of an infant’s claim given years of future medical needs, have no cap.
As Texas NICU IV extravasation lawyers, we build each case with the child’s entire future in mind. Compensation is not just about addressing what has already happened. It is about ensuring the resources are in place for every surgery, therapy session, and form of care your child may need as they grow.
Texas Laws Impacting Your Claim
Texas law imposes strict requirements on medical malpractice claims, including a two-year statute of limitations (with special provisions for minors) and the mandatory filing of an expert report within 120 days of each defendant’s original answer.
The statute of limitations generally requires a claim to be filed within two years of the date the injury occurred or was discovered. For minors under the age of 12, the statute provides until the child’s 14th birthday to file or have a claim filed on their behalf. Parents’ claims for a minor’s medical expenses, however, are still subject to the standard two-year deadline, which is why early consultation with a NICU malpractice lawyer in Texas matters.
Before filing a lawsuit, Texas law also requires a pre-suit notice letter to be sent to each healthcare provider at least 60 days before the case is filed. This requirement is outlined in Texas Civil Practice and Remedies Code § 74.051 and is designed to give the provider an opportunity to respond before litigation begins. This notice period allows the hospital’s insurance carrier to investigate the claim. However, it rarely leads to a settlement offer without the pressure of a lawsuit.
Chapter 74 Expert Reports
One of the most important deadlines in a Texas medical malpractice case is the 120-day expert report requirement. Within 120 days of each defendant’s original answer, the plaintiff must serve that defendant with a written report from a qualified expert witness. This report must identify the applicable standard of care, explain how the provider breached that standard, and describe how the breach caused the injury.
This statute is strictly enforced. Even a minor technical error in the report can lead to dismissal. Securing a comprehensive Texas 120-day expert report is a priority for our legal team immediately upon reviewing your case. At Hastings Law Firm, we identify and retain qualified experts early in the process so that this critical deadline is never at risk.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
If your child suffered a preventable IV injury in the NICU, you do not have to face the hospital’s legal team on your own. Hastings Law Firm was built for cases exactly like this. Our team includes former defense attorneys who understand how hospitals respond to these claims, in-house nurses who can interpret your child’s medical records, and a national network of neonatology experts ready to support your case.
Our founder, Tommy Hastings, is board-certified in Personal Injury Trial Law, a distinction held by less than 2% of Texas attorneys. He has spent nearly two decades holding healthcare providers accountable for preventable harm. We prepare every case as though it will go to trial, and that preparation allows us to negotiate from a position of strength.
As Texas NICU IV extravasation lawyers, we are ready to review what happened, explain your options, and help you take the first step toward answers and accountability. Contact us today for a free, confidential case evaluation. There is no fee unless we win.
Frequently Asked Questions About NICU IV Extravasation in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
