

Texas Infant Opioid Oversedation Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Neonatal opioid medication errors in the NICU can cause rapid respiratory suppression and lasting brain injury when dosing, pump settings, monitoring, or communication fails. These events often involve preventable breakdowns such as decimal point mistakes, infusion pump misprogramming, and missed alarms during critical moments. Accountability can be complex because responsibility may involve multiple providers and the hospital, and key digital records can be overwritten if not preserved. If you or a loved one were harmed or worse due to infant opioid oversedation in Texas, contact Hastings Law Firm for a free, confidential case review.
Top Rated Texas Medical Attorneys for Neonatal Medication Errors
What You Should Know About Neonatal Pain Medication Error Claims in Texas:
- Life altering harm can occur when opioid oversedation suppresses an infant breathing and is not corrected quickly.
- Permanent brain injury risk can rise when monitoring is not actively watched or alarms are silenced or set incorrectly.
- Accountability can involve multiple defendants because prescribing, pharmacy, nursing, and hospital systems can each contribute to a medication error.
- Options can be lost if a required early expert report is not served because Texas courts can dismiss the case permanently.
- Recovery can be limited for non economic losses because Texas law generally caps pain and suffering damages.
- Long term financial needs can remain fully compensable because Texas medical malpractice law does not cap economic damages.
- Proof can become harder if digital medication data is overwritten because infusion pump logs and dispensing records may be stored only temporarily.
- Disputes can turn on documentation gaps because some emergency events are not fully captured in the medical record.

A Healthcare Focused Law Firm
When an infant suffers harm from an opioid medication error, the weight of that experience can feel impossible to carry. You may be searching for answers about what went wrong and whether anyone will be held accountable. As a Texas infant opioid oversedation lawyer, we focus exclusively on medical malpractice cases, including neonatal medication errors that cause serious injury or death. Our legal and medical team, which includes in-house nurse consultants and former defense attorneys, investigates these cases from day one with the goal of uncovering the truth.
If your child was harmed by a dosing error or drug administration failure in the NICU, we can review what happened and explain your legal options. Contact us for a free, confidential case evaluation.
Common Causes of Opioid Oversedation in the NICU
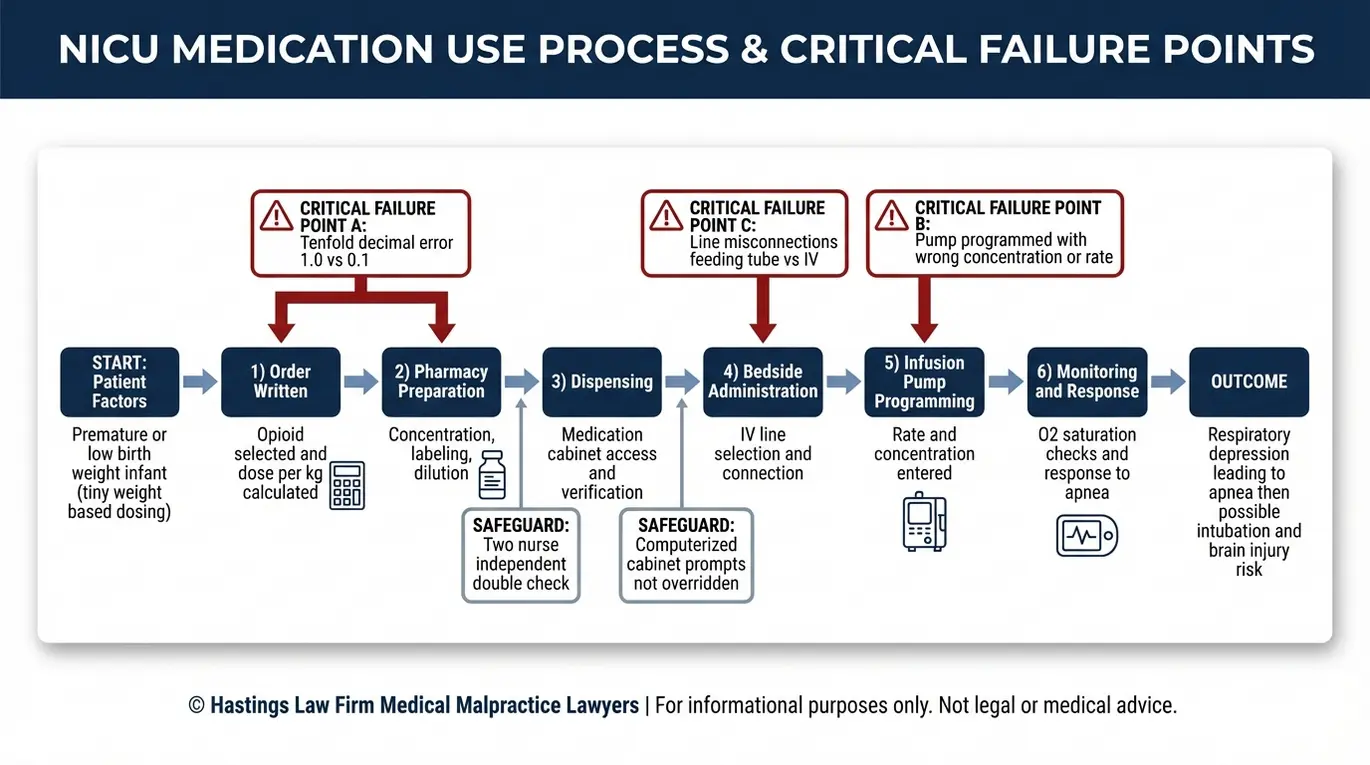
Opioid oversedation in the NICU is typically caused by calculation errors, specifically “tenfold” decimal point mistakes, improper programming of infusion pumps, or communication failures during shift changes. Opioids are powerful medications used for pain relief that require extreme precision when administered to newborns. These errors are preventable, and they tend to follow recognizable patterns that an experienced NICU medication error lawyer can identify through a detailed records review.
Infants treated in a neonatal intensive care unit (NICU), the specialized hospital ward designed to care for critically ill or premature newborns, receive medications at doses measured in micrograms or fractions of a milligram. The margin for error is extraordinarily small. When opioids like fentanyl or morphine are involved, even a minor miscalculation can suppress an infant’s breathing and lead to catastrophic injury.
There are several well-documented failure points in the NICU medication process. Each represents a moment where a safety check should have caught the error but did not.
Dosage calculation errors are the most frequent cause of infant opioid overdose. A provider may calculate the dose based on a standard adult formula and fail to adjust for the infant’s actual weight. In other cases, a decimal point is misplaced during the math, turning a safe dose of 0.1 mg into a dangerous dose of 1.0 mg. For a premature infant weighing less than two pounds, this kind of tenfold dosing error can be life-threatening.
Infusion pump programming errors occur when a nurse or technician enters incorrect values into the pump that controls the intravenous delivery rate. An infusion pump programming error, which is a mistake in the settings that regulate how fast and how much medication flows through the IV, can deliver an entire dose in minutes rather than hours. These errors sometimes go undetected until the infant shows signs of respiratory distress.
Line misconnections represent another critical equipment failure in the crowded NICU environment. Infants are often connected to multiple tubes, including intravenous lines for medication and enteral tubes for feeding. A line misconnection occurs when a nurse mistakenly attaches an IV line to a feeding tube or vice versa. This can result in opioid medication being delivered via the wrong route or incompatible fluids mixing in the bloodstream, leading to immediate toxicity or embolism.
Communication breakdowns during handoffs between nursing shifts or between the prescribing physician and the administering nurse can introduce dangerous gaps. If the outgoing nurse does not clearly communicate the current dosage, the infusion rate, or recent changes to the medication order, the incoming nurse may administer a second dose or continue an incorrect rate. In the high-stress environment of a NICU, verbal orders given during an emergency are particularly prone to misinterpretation if not immediately verified and documented.
Bypassed safety protocols also contribute to neonatal overdose events. Many NICUs use computerized medication dispensing cabinets that generate alerts when a dose falls outside the expected range. Staff may override these alerts, particularly during high-volume shifts or when understaffing creates pressure to move quickly. Similarly, two-nurse verification protocols, where a second nurse independently checks the dose before administration, are sometimes skipped. “Alarm fatigue” can also lead to errors, where staff become desensitized to constant equipment beeping and fail to respond to a critical pump alert in time.
| Risk Factor | How It Leads to Oversedation |
|---|---|
| Tenfold (decimal point) dosing error | A misplaced decimal multiplies the intended dose by 10x, overwhelming the infant’s system |
| Infusion pump misprogramming | Incorrect rate or concentration settings deliver too much drug too fast |
| Line misconnection | Medication is delivered via the wrong route (e.g., IV to feeding tube) due to tubing confusion |
| Shift-change communication failure | Critical dosing information is lost between providers, leading to duplicate or incorrect doses |
| Override of electronic safety alerts | Computerized warnings about out-of-range doses are dismissed without review |
| Skipped two-nurse verification | The required independent dose check by a second nurse does not occur |
| Weight-based calculation error | The dose is calculated using an incorrect weight or an adult-based formula |
An infant opioid overdose attorney examines each of these failure points to determine where the process broke down. At Hastings Law Firm, our in-house medical staff reviews pharmacy logs, pump data, and nursing documentation to reconstruct exactly what was ordered, what was dispensed, and what was administered.
Tenfold Dosing Errors in Low Weight Infants
The tenfold dosing error, a mistake where a decimal point is misplaced and the intended dose is multiplied by ten, is especially dangerous for micro-preemies. Micro-preemies, extremely low birth weight infants typically weighing less than 750-800 grams (under 2 pounds), require drug administration precision down to the microgram.
Consider how the math works. If a physician prescribes 0.05 mg of morphine for an infant weighing 800 grams, and a pharmacist or nurse mistakenly prepares 0.5 mg, the infant receives ten times the safe amount. The infant’s immature liver and kidneys cannot metabolize or clear the excess opioid quickly enough, and respiratory depression can begin within minutes.
These prescription errors are not rare. They are one of the most commonly reported medication errors in neonatal care. Neonatal overdose lawyers look specifically at the chain of documentation, from the original order to the pharmacy preparation to the bedside administration record, to identify where the decimal error was introduced and who failed to catch it.
Medical Negligence Standards for Infant Opioid Administration
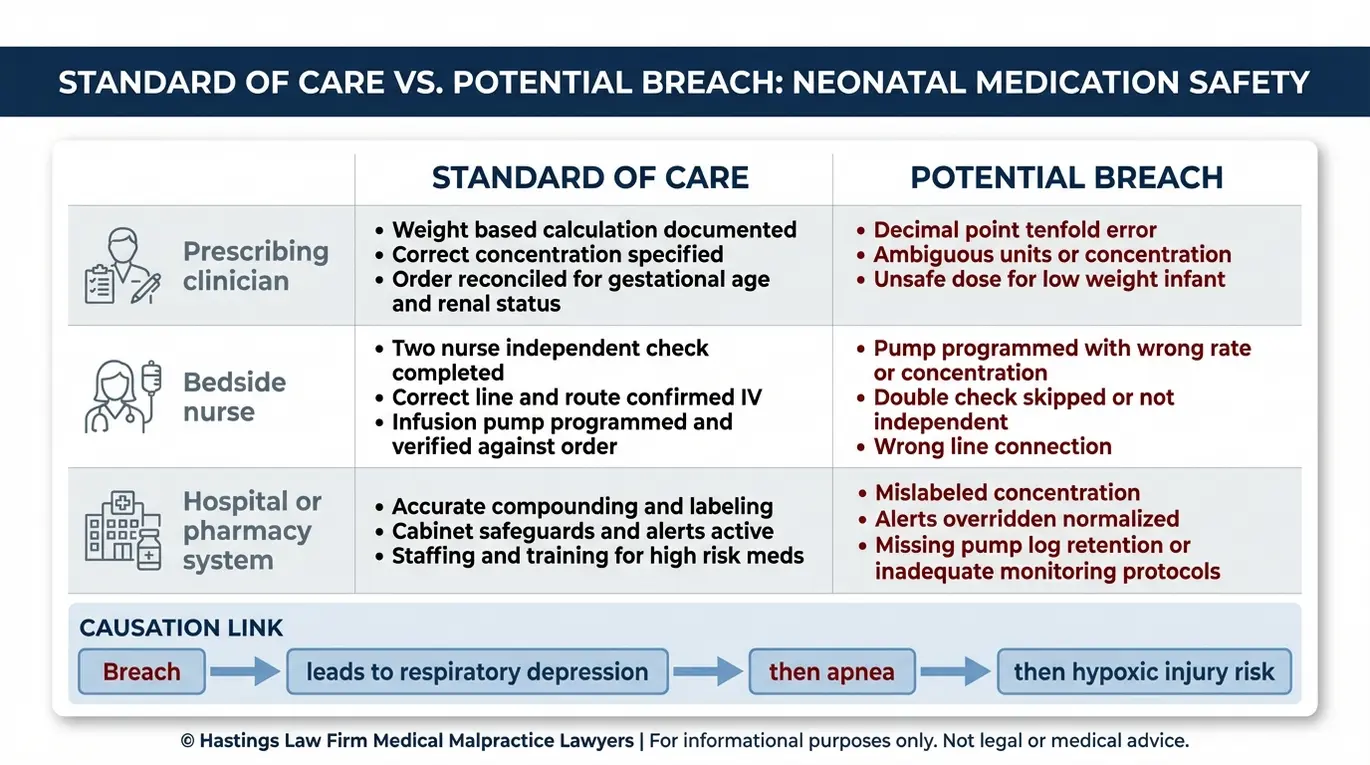
To prove negligence in an infant oversedation case, a Texas malpractice attorney for infants must demonstrate that the medical provider deviated from the accepted standard of care, directly causing respiratory distress or brain injury. Medical negligence occurs when a healthcare professional’s actions fall below the standard of care expected of a reasonably competent provider. Our founder, Tommy Hastings, is board-certified in personal injury trial law, a distinction held by fewer than 2% of Texas attorneys.
The standard of care for opioid administration in the NICU includes a series of protocols designed to prevent oversedation and detect it immediately if it occurs. When these protocols are followed, opioid-induced respiratory depression, a condition where the drug suppresses the brain’s signal to breathe, can usually be identified and reversed before permanent harm occurs.
A standard of care checklist in these cases typically includes:
- Weight-based dosing verified by two independent providers before administration
- Correct programming of the infusion pump confirmed by a second nurse
- Continuous pulse oximetry and cardiorespiratory monitoring during and after opioid delivery
- Immediate bedside availability of naloxone (the opioid reversal agent)
- Documented reassessment of the infant’s respiratory status at defined intervals after each dose
- Clear communication of the current medication regimen at every shift change
When any of these steps is missed, the risk of a preventable injury increases significantly.
Monitoring failures are among the most common forms of negligence our opioid error law firm investigates. If an infant’s oxygen saturation drops after receiving an opioid and no one is watching the monitor, or if the alarms have been silenced or set to incorrect thresholds, precious minutes pass without intervention. Those minutes can mean the difference between a full recovery and permanent brain damage.
Standard of care requires not just the presence of monitoring equipment, but active surveillance. Nurses must respond to alarms immediately rather than assuming they are false positives. In many cases we handle, the central monitoring station records show prolonged periods of desaturation that went unaddressed because staff were distracted or not present at the bedside.
Response failures compound monitoring breakdowns. When an infant enters apnea, a condition where breathing stops entirely, the standard of care generally requires immediate intervention. This may include stimulation, bag-mask ventilation, intubation (placing a breathing tube), or mechanical ventilation.
A delayed response to apnea after opioid administration can deprive the brain of oxygen long enough to cause hypoxic-ischemic encephalopathy. Rapid intervention is critical in neonatal care. A delay of even a few minutes in administering naloxone or providing ventilation can lead to irreversible cellular damage in the brain.
Liability in these cases often involves more than one provider. The prescribing physician may bear liability for ordering an incorrect dosage. The administering nurse may be liable for a pump programming error or for failing to perform the required two-nurse check.
The hospital itself may be liable for pharmacy errors, inadequate staffing levels, or failure to enforce its own safety protocols. For instance, if a hospital knows that its nurses are consistently bypassing safety checks due to understaffing and fails to correct the issue, the institution itself may be directly negligent. When suing for NICU overdose, our legal team evaluates each provider’s role separately to build the strongest possible case, often naming multiple defendants to ensure all contributing factors are addressed.
At Hastings Law Firm, we work with qualified medical experts in neonatology, pharmacology, and nursing to evaluate whether the care provided met the standard. Our team includes former defense attorneys who understand how hospitals prepare their responses, and in-house nurses who can interpret charting patterns and identify inconsistencies that might otherwise be overlooked.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Understanding Texas Law and the Expert Report Requirement
Texas law requires plaintiffs to serve an expert report detailing the standard of care, the breach, and causation within 120 days of filing suit, or the case will be dismissed with prejudice. Legal standards in Texas are shaped by specific tort reform laws that require detailed evidence early in the litigation process. With over two decades of experience, we have focused our practice exclusively on medical malpractice litigation to provide the specialized knowledge these cases require.
The requirement comes from the Texas Medical Liability Act (TMLA), a piece of Texas tort reform legislation that imposes procedural hurdles that do not exist in most other types of civil litigation. Under the TMLA, a plaintiff’s attorney must hire a qualified medical expert to review the case. This expert produces a written report detailing exactly what the provider should have done and how their actions caused the child’s injury. If the report is late, incomplete, or fails to meet the legal standard, the court can dismiss the case permanently.
This 120-day clock starts on the date the lawsuit is filed. For families still processing what happened to their child, that deadline can arrive quickly. An experienced infant injury legal team will begin lining up expert support during the investigation phase, well before the suit is even filed, so the report is ready when it is needed.
The quality of the expert report matters as much as the timing. Texas courts have addressed what qualifies as an adequate report, and the standard has real consequences. In *Johnson v. Marks* (Texas Supreme Court), the court examined the sufficiency of expert reports under the TMLA and reinforced that the report must provide enough detail to inform the defendant of the specific conduct at issue. A vague or conclusory report will not survive a challenge. The Expert Institute’s overview of Texas expert witness report rules provides a helpful summary of these requirements for families trying to understand the process.
The role of proper documentation is critical. In cases where medical records are incomplete or silent on key events, the Texas Supreme Court decision in *Loaisiga v. Cerda* becomes highly relevant. This precedent establishes how expert reports may, in certain circumstances, rely on the plaintiff’s factual assertions when the hospital’s own documentation fails to capture the negligence. This is vital in NICU cases where charting gaps often exist during emergency resuscitation events.
Evidence preservation is equally urgent. Infusion pump logs, electronic medication dispensing records, and pharmacy audit trails are stored digitally, and many hospital systems overwrite or purge this data on a set schedule. If these records are lost, it becomes much harder to prove what medication was actually delivered and at what rate. Our team sends preservation letters to the hospital immediately upon engagement to protect this data before it disappears.
This is one of the reasons families should consult with a Texas infant opioid oversedation lawyer as early as possible, even if they are not yet sure they want to file a lawsuit. The investigation phase is about gathering facts. Once digital records are gone, they cannot be reconstructed.
Calculating Damages for Hypoxic-Ischemic Encephalopathy
Damages for HIE caused by oversedation include economic costs for lifetime medical care, such as nursing, therapy, and equipment, and non-economic damages for pain, suffering, and physical impairment. Legal damages refer to the financial compensation paid to a family to cover the losses caused by a preventable medical error. These funds help provide the necessary support for a child who has suffered a life-altering injury.
Hypoxic-ischemic encephalopathy (HIE), a type of brain injury caused by reduced oxygen and blood flow to the brain, occurs when an opioid overdose suppresses an infant’s breathing and the condition is not corrected quickly. The resulting oxygen deprivation can cause HIE or, in more severe cases, anoxic encephalopathy, a broader form of brain damage caused by a complete loss of oxygen. The severity of the injury depends largely on how long the brain went without adequate oxygen and how quickly medical intervention restored normal breathing.
Children who survive HIE may face cerebral palsy, seizure disorders, developmental delays, cognitive impairment, or a combination of these conditions. Many will require around-the-clock nursing care, ongoing physical and occupational therapy, adaptive equipment, and specialized educational support throughout their lives.
Economic damages cover the measurable financial costs of these needs. There is no cap on economic damages in Texas medical malpractice cases, which means compensation for infant brain injury can reflect the true, projected cost of care. Economic damages in an HIE case typically include:
- Past and future medical expenses, including hospitalizations, surgeries, and specialist care
- Home nursing and attendant care costs
- Physical, occupational, and speech therapy
- Adaptive equipment such as wheelchairs, communication devices, and modified vehicles
- Prescription medications
- Lost earning capacity over the child’s expected working lifetime
- Home modifications for accessibility
To calculate these figures accurately, our overdose lawsuit damages team works with life care planners and forensic economists. A life care plan is a detailed, year-by-year projection of every medical service, therapy session, and piece of equipment the child will need from the present through their expected lifespan. For a child with severe HIE, this plan might include costs for a modified van, ceiling track lifts for the home, 24-hour LVN care, and replacement schedules for wheelchairs every five years. An economist then assigns present-day dollar values to those future costs, accounting for inflation and medical cost growth to ensure the settlement funds last for the child’s entire life.
Non-economic damages compensate the child and family for pain, suffering, mental anguish, and physical impairment. Under Texas tort reform, as outlined in the Texas Civil Practice and Remedies Code, Section 74.301, non-economic damages are generally capped at $250,000 per individual provider or $500,000 for institutional defendants. While these caps limit one category of recovery, they do not restrict the economic damages that often make up the largest portion of HIE settlements in Texas.
Wrongful death damages may apply if the infant did not survive. Texas law allows parents to pursue compensation for the loss of companionship, mental anguish, and the economic contributions the child would have made over a lifetime. While no legal remedy can truly compensate for the loss of a child, a wrongful death claim can provide a measure of justice and financial stability for the grieving family.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
No amount of money can undo what happened to your child. But a successful claim can secure the resources your family needs to provide the best possible care going forward. As a medical malpractice firm, we focus on helping families secure the resources needed for future care. As a Texas infant opioid oversedation lawyer, Hastings Law Firm has the medical and legal team to investigate what went wrong and hold the responsible parties accountable.
We work on a contingency fee basis, which means you pay no attorney fees or costs unless we recover compensation for your family. There is no financial risk in reaching out.
If your infant was harmed by a medication error in the NICU, call us or complete our online form to start a free, confidential case evaluation. We are here to listen, answer your questions, and help you understand your options.
Frequently Asked Questions About Infant Opioid Oversedation in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
