

Texas Infant Intubation Injury Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Infant intubation and ventilator errors in the NICU can leave families facing lasting harm and overwhelming uncertainty. Problems like misplaced breathing tubes, delayed airway support, or improper ventilation settings can reduce oxygen delivery and cause serious injury to the brain, lungs, and other organs. Understanding what went wrong often depends on whether the care team followed accepted neonatal resuscitation protocols and confirmed tube placement and ventilation effectiveness. If you or a loved one were harmed or worse due to infant intubation injury in Texas, contact Hastings Law Firm for a free, confidential case review.

Top Rated Birth Injury Attorneys Helping Families Across Texas
What You Should Know About Neonatal Ventilation Negligence Claims in Texas:
- Lifelong injury can result when intubation or ventilation errors reduce oxygen delivery during neonatal resuscitation.
- Severe brain injury can follow when a breathing tube is placed in the esophagus and the mistake is not promptly recognized.
- Lasting airway damage can occur when the wrong tube size is used or when repeated insertion attempts cause trauma.
- Permanent lung complications can develop when ventilator pressures are set too high and fragile lung tissue ruptures.
- Additional brain injury risk can arise when overventilation drives carbon dioxide too low and reduces blood flow to vulnerable brain tissue.
- Options for financial recovery can be limited by caps on non economic damages in Texas medical malpractice cases.
- Long term care costs can remain recoverable because Texas law does not cap economic damages for documented medical needs.
- Disputes about responsibility can involve physicians, hospitals, and respiratory therapists when multiple providers participate in airway management.
- Missing or inconsistent charting can complicate accountability because absent ventilator logs or capnography readings may indicate critical steps were skipped.
- Establishing a clear timeline can be central because ventilator logs, blood gas results, imaging, and EMR audit trails may show what occurred and when.

A Healthcare Focused Law Firm
When a newborn suffers an injury during intubation or ventilator management, parents are often left searching for answers while coping with fear and uncertainty. You may sense that something went wrong in the NICU but feel unsure how to confirm it or what to do next. That instinct matters, and you deserve clarity about what happened and whether it was preventable.
As a Texas Infant Intubation Injury Lawyer team, we focus exclusively on medical malpractice. Our attorneys work alongside in-house nurse consultants, nationally recognized medical experts, and Board Certified Patient Advocates to investigate neonatal airway injuries. We determine whether the care your child received fell below accepted standards. If your family is facing this situation, we can review the medical records, explain your options, and help you understand the path forward at no cost to you.
Common Neonatal Resuscitation and Intubation Errors
Neonatal intubation errors often involve placing the breathing tube into the esophagus instead of the trachea, selecting the wrong tube size, or causing physical trauma to the airway during repeated insertion attempts. These mistakes can happen in seconds, but their consequences may last a lifetime.
When a newborn cannot breathe on its own, the medical team must secure an airway quickly and correctly. This typically involves inserting an endotracheal tube (ETT), a small plastic tube placed through the mouth or nose and into the windpipe (trachea) to deliver oxygen directly to the lungs. The procedure demands precision, especially in premature or critically ill infants whose airways are extremely small and fragile. Even a minor deviation in technique can cause catastrophic damage to the surrounding tissues or fail to provide the necessary oxygen to the brain.
Errors during neonatal resuscitation can take several forms:
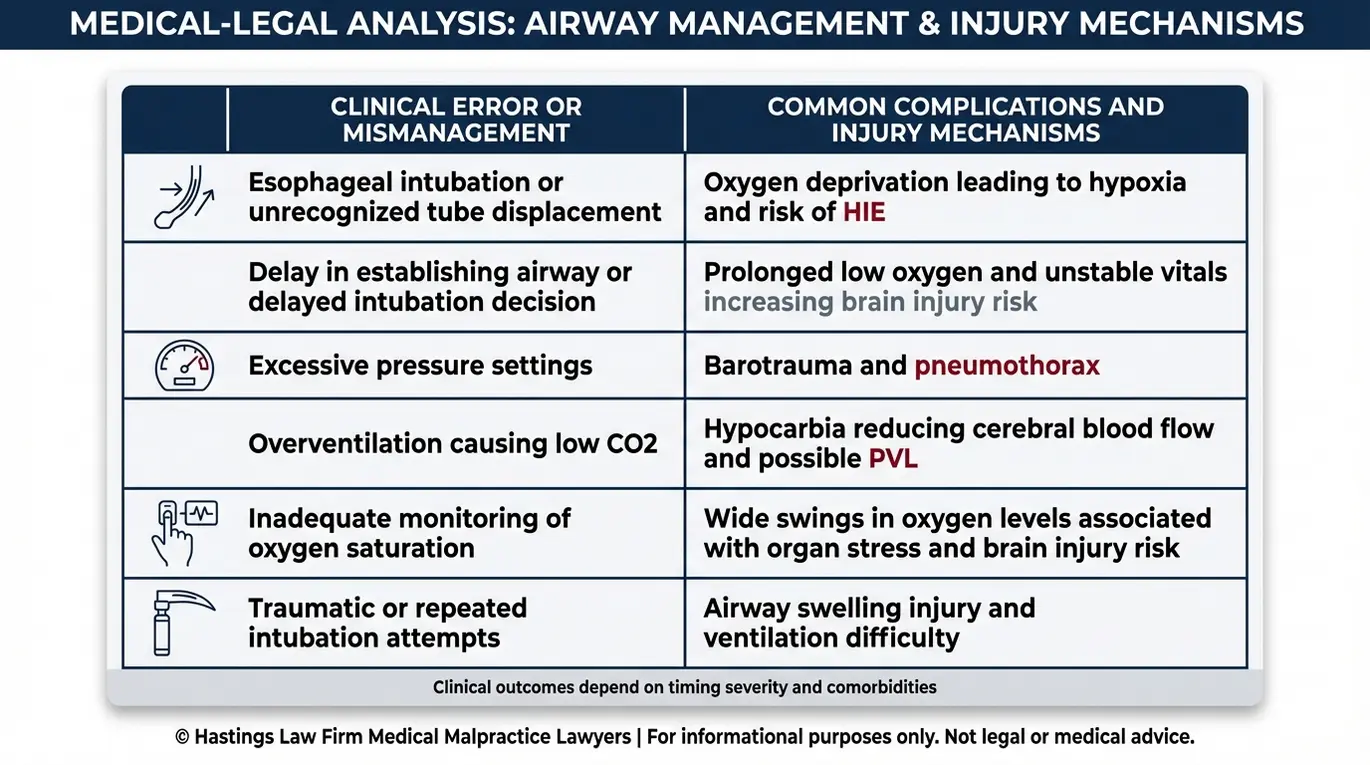
- Esophageal intubation: This occurs when the endotracheal tube is mistakenly placed into the esophagus, the tube leading to the stomach, rather than the trachea. When this happens, oxygen never reaches the lungs. If the misplacement is not detected and corrected quickly, the infant can suffer severe oxygen deprivation within minutes. This error is often indicated by a lack of breath sounds, absence of CO2 return, or stomach distension.
- Wrong tube size: Selecting a tube that is too large can damage the vocal cords and tracheal lining, leading to stenosis, which is a narrowing of the airway, or scarring. In contrast, a tube that is too small may fail to deliver adequate ventilation. This allows air to leak around the tube and reduces the amount of oxygen that actually reaches the lungs.
- Excessive or repeated insertion attempts: Each failed intubation attempt can cause swelling, bleeding, or trauma to the infant’s delicate airway structures. Swelling from repeated attempts can make the airway progressively harder to access. This creates a cycle that worsens the emergency and increases the risk of hypoxic injury.
- Delayed intubation: When a distressed infant shows clear signs of respiratory failure, and the team waits too long to intubate, the result can be devastating. These signs include persistent cyanosis, low heart rate, or poor tone. Even a short delay can result in severe metabolic acidosis and hypoxia, a dangerous drop in oxygen that can injure the brain and other organs.
- Failure to confirm placement: After insertion, the medical team must verify that the tube is correctly positioned in the trachea. Skipping or improperly performing this confirmation step, such as failing to use a colorimetric CO2 detector, is one of the most preventable errors in neonatal airway management.
Not every difficult intubation rises to the level of medical malpractice. Some infants have anatomical challenges, such as micrognathia or subglottic stenosis, that make the procedure genuinely difficult. The distinction lies in whether the medical team followed accepted protocols, recognized complications promptly, and responded appropriately. A Texas infant intubation injury lawyer helps families distinguish between unavoidable complications and preventable negligence.
As an infant intubation attorney team, we work with neonatal specialists to reconstruct the timeline of events and determine whether the care team’s actions met the required standard. A neonatal malpractice lawyer evaluates not just what happened, but what should have happened based on the infant’s condition and the resources available at the time.
Dangers and Complications of Improper Ventilation
Improper ventilation can lead to severe complications such as hypoxic-ischemic encephalopathy (HIE), a type of brain injury caused by combined oxygen deprivation and reduced blood flow; lung collapse, known medically as a pneumothorax; and permanent brain damage caused by unstable oxygen levels.
The consequences of ventilation errors depend on how long the infant was deprived of adequate oxygen and how correctly the ventilator was managed. Some complications develop within minutes. Others emerge over days or weeks as the full scope of the injury becomes apparent. One critical risk is barotrauma, which occurs when ventilator pressures are set too high for the infant’s lung capacity.
This excessive pressure can rupture the fragile alveoli, which are the tiny air sacs in the lungs where oxygen exchange occurs. Ruptured alveoli can cause air to leak into the chest cavity and potentially collapse the lung. This requires the immediate insertion of a chest tube to re-expand the lung and stabilize breathing.
| Complication | Cause | Potential Long-Term Impact |
|---|---|---|
| Hypoxic-ischemic encephalopathy (HIE) | Prolonged oxygen deprivation during failed intubation or misplaced tube | Cerebral palsy, cognitive disabilities, seizure disorders |
| Pneumothorax (collapsed lung) | Excessive ventilator pressure rupturing fragile lung tissue | Respiratory distress, need for chest tube, chronic lung problems |
| Barotrauma | Ventilator pressures set too high for the infant’s lung capacity | Structural lung damage, prolonged NICU stay |
| Bronchopulmonary dysplasia (BPD) | Extended mechanical ventilation with improper settings | Chronic lung disease requiring long-term oxygen therapy |
| Cerebral palsy | Sustained hypoxia or unstable oxygenation during the neonatal period | Lifelong motor impairment, developmental delays |
According to Data and Statistics for Cerebral Palsy from the CDC, cerebral palsy is one of the most common motor disabilities in childhood. Many cases are associated with events around the time of birth, including oxygen deprivation caused by airway management failures.
An intubation injury lawyer in Texas can help families connect these clinical events to specific deviations from the standard of care. Under Texas Civil Practice and Remedies Code Chapter 74, medical malpractice claims require proof that a healthcare provider’s negligence directly caused the patient’s injury. A neonatal ventilation negligence attorney works with medical experts to build that causal link between what went wrong and the harm your child experienced.
Overventilation and White Matter Injury
One of the lesser-known risks of mechanical ventilation is overventilation, which occurs when the ventilator delivers breaths too rapidly or at excessive volumes. This can drive the infant’s carbon dioxide levels dangerously low, a condition called hypocarbia, meaning abnormally reduced CO2 in the blood.
Carbon dioxide helps regulate blood flow to the brain. When CO2 drops too low, blood vessels in the brain constrict, reducing the oxygen supply to vulnerable areas of white matter. This can lead to periventricular leukomalacia (PVL), a form of brain injury involving damage to the white matter surrounding the brain’s ventricles.
PVL is a recognized cause of cerebral palsy and cognitive impairment in premature infants. Because the damage occurs at the cellular level, it may not be immediately obvious on early imaging. We evaluate ventilator logs, blood gas results, and the timing of neuroimaging studies to determine whether overventilation contributed to the injury.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Standard of Care for Neonatal Airway Management
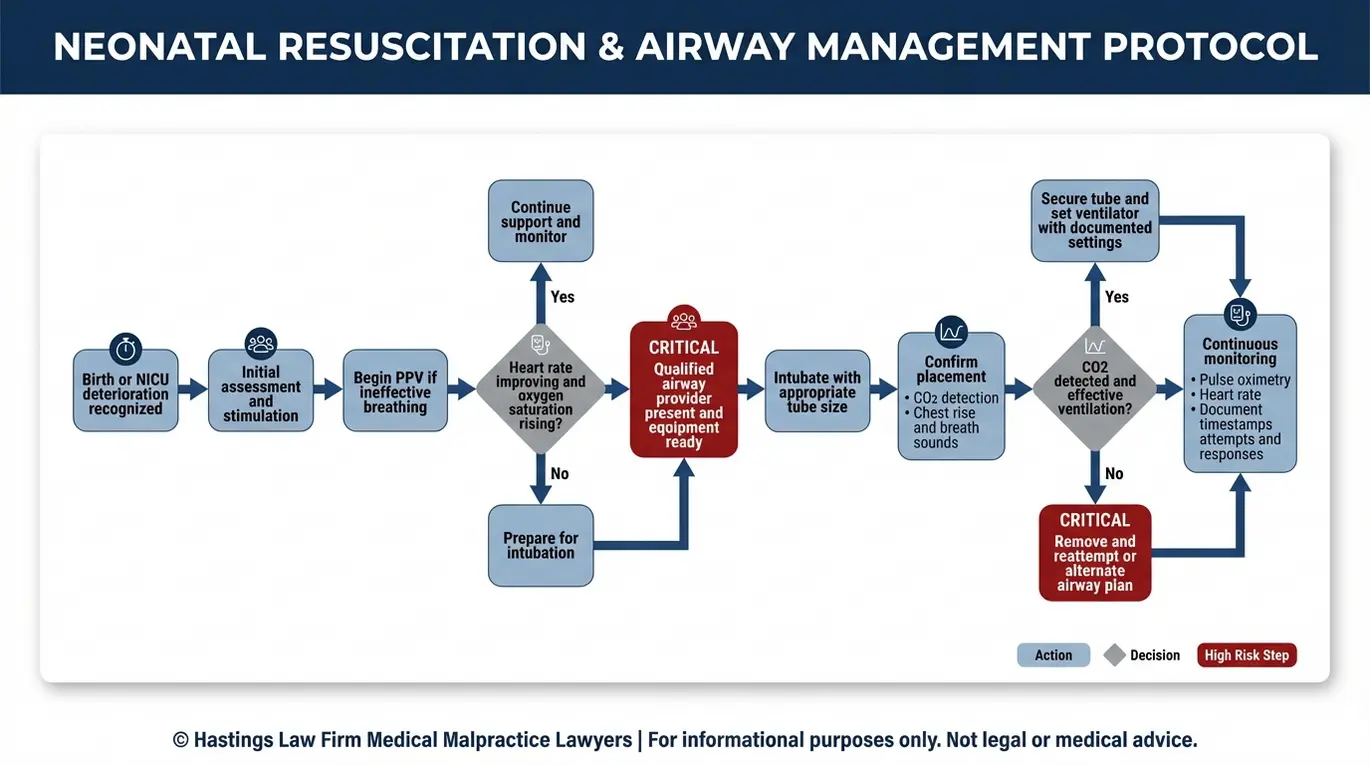
The standard of care requires medical providers to follow the Neonatal Resuscitation Program (NRP) protocols, a set of evidence-based guidelines that establish specific timelines for intubation, confirmation of tube placement using CO2 detection, and continuous monitoring of the infant’s vital signs.
The Neonatal Resuscitation Program (NRP), developed jointly by the American Academy of Pediatrics and the American Heart Association, is the universal benchmark for neonatal resuscitation. Hospitals are expected to train their delivery and NICU staff in NRP protocols. They must ensure that qualified personnel are present at every delivery where complications are anticipated.
According to the Updated 2025 Neonatal Resuscitation Guidelines from Hope for HIE, the most recent NRP revisions continue to emphasize rapid assessment and early intervention. They also focus on structured decision-making during the critical first minutes of life.
The NRP protocol generally follows a structured sequence of steps. When we evaluate a case as a Texas infant intubation injury lawyer team, we compare the documented care against these benchmarks:
- Initial assessment of the newborn’s breathing, heart rate, and tone immediately after delivery, including assigning an Apgar score (a measure of physical condition) to evaluate overall status
- Stimulation and airway clearance if the infant is not breathing effectively
- Initiation of positive pressure ventilation (PPV), the delivery of air or oxygen into the lungs using a mask and bag, if the heart rate remains below 100 beats per minute
- Continuous pulse oximetry monitoring to track oxygen saturation levels throughout resuscitation
- Intubation if PPV does not produce an adequate response within the recommended timeframe
- Confirmation of endotracheal tube placement using a CO2 detector before initiating mechanical ventilation
- Ongoing heart rate and oxygen monitoring with documented reassessments at defined intervals
Each step builds on the previous one. Skipping a step, performing it out of sequence, or failing to document the response at each stage can constitute a breach of the standard of care.
A birth injury attorney Texas families trust examines whether the team had the right personnel, equipment, and training to manage the resuscitation. Hospitals have an obligation to ensure that staff are NRP-certified and that resuscitation equipment is immediately available. This includes ensuring that the team is capable of advanced airway management if the primary provider fails to secure the airway. Such situations necessitate a rescue protocol that must be executed without delay.
Confirming Tube Placement and Depth
One of the most critical steps after intubation is verifying that the endotracheal tube is correctly positioned in the trachea and inserted to the proper depth. Failure to confirm placement is a leading cause of preventable neonatal injury.
The standard method for confirmation is end-tidal carbon dioxide monitoring, also called capnography, which detects CO2 in the infant’s exhaled breath. If CO2 is present, the tube is in the trachea. If no CO2 is detected, the tube may be in the esophagus, and the team must act immediately.
Tube depth is guided by the Lip-to-Tip rule, a calculation based on the infant’s weight or gestational age. It determines how far the tube should be inserted. Placing the tube too deep can result in one-sided lung ventilation, where only one lung receives air. Placing it too shallow increases the risk of accidental dislodgement.
We review capnography data, chest X-rays taken after intubation, and nursing documentation to evaluate whether these confirmation steps were performed correctly and in a timely manner.
Establishing Liability for Ventilator and Intubation Injuries
Liability is established by proving that the physician, respiratory therapist, or hospital staff deviated from accepted medical standards, and that this deviation directly caused the infant’s injury. In medical malpractice, establishing liability means identifying which party is legally responsible for the harm caused by negligence.
As a Texas infant intubation injury lawyer team, we investigate multiple layers of potential responsibility. Neonatal airway management involves several providers working simultaneously. Our legal team includes former defense attorneys who previously worked for hospital systems, providing us with insider insight into how these entities challenge medical negligence claims.
Physician liability arises when the attending physician or neonatologist fails to follow NRP protocols, delays a necessary intubation, or does not respond appropriately to deteriorating vital signs. Whether the physician is a hospital employee or an independent contractor can affect which entities are legally responsible for their negligence.
Hospital and institutional liability may exist when the facility itself contributed to the conditions that caused the injury. This includes situations where staffing levels were inadequate, equipment was not properly maintained, or hospital policies failed to ensure that NRP-certified personnel were available. Under Texas law, hospitals can be held directly liable for their own institutional negligence.
Respiratory therapist liability is an important element. Under the Texas Occupations Code Chapter 604, respiratory care practitioners have an independent professional duty. If a respiratory therapist follows a ventilator order that is clearly unsafe, that therapist may bear individual responsibility. Therapists must use the chain of command to protect the patient.
Documentation failures can also support a negligence claim. Gaps in the electronic medical record (EMR) often raise important questions. Missing ventilator logs or absent capnography readings may suggest that critical steps were skipped.
Modern EMR systems contain audit trails that track exactly when and by whom a record was accessed. Our in-house medical staff, including nurse consultants and Board Certified Patient Advocates, are trained to identify these charting inconsistencies and metadata anomalies.
We build a detailed timeline from the medical records, comparing every documented action and omission against the standard of care. Expert testimony from qualified neonatologists and respiratory specialists then connects those deviations to the specific injuries the child suffered.

Recovering Damages for Lifelong Neonatal Injuries
Recoverable damages in infant intubation injury cases include current and future medical expenses, costs for life care planning, pain and suffering, and compensation for the child’s loss of earning capacity. Recovering damages refers to the financial compensation meant to address the lifelong needs of a child injured at birth.
Economic damages cover the measurable financial costs associated with the injury. These typically include:
- Past and future medical bills, including surgeries, hospitalizations, and specialist visits
- Rehabilitation costs such as physical therapy, occupational therapy, and speech therapy
- Specialized equipment including wheelchairs, adaptive devices, and home modifications
- In-home nursing care or attendant care services
- Educational support and special needs accommodations
- Loss of the child’s future earning capacity
- Compensation for birth injury related expenses that arise unexpectedly as the child matures
For children diagnosed with conditions like cerebral palsy or cognitive impairment resulting from oxygen deprivation, these costs can be substantial. Texas law does not cap economic damages. Families can recover the full documented cost of care, both past and projected. This includes accounting for medical inflation to ensure funds are sufficient for treatments decades in the future.
Non-economic damages compensate for losses that cannot be easily measured in dollars. These include the child’s physical pain and suffering, physical impairment, disfigurement, and loss of enjoyment of life. While Texas does impose caps on non-economic damages in medical malpractice cases, the economic component of the claim remains uncapped.
Life care plans are essential in cases involving permanent disability. A life care plan is a detailed document prepared by a qualified expert that projects every category of care the child will need over their expected lifespan. According to Pediatric Rehab Consultants’ resource on Life Care Planning for Youth with Disabilities, these plans address medical treatment, therapy, equipment, housing, and transportation needs across the individual’s lifetime.
As a Texas infant intubation injury lawyer team, we retain life care planning specialists, economists, and medical experts early in the case. Expert testimony ties each projected cost back to the specific injuries caused by negligence. This helps make the damages claim both credible and complete.
In cases where an infant dies as a result of intubation or ventilator errors, families may pursue a wrongful death claim. These cases carry their own legal requirements under Texas law. We can explain how those claims work during a confidential consultation.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
If your child suffered an airway injury in the NICU that you believe was preventable, our team is here to help you understand what happened and what options may be available.
Hastings Law Firm brings together board-certified trial attorneys and in-house medical professionals who focus entirely on medical malpractice. Founded by Tommy Hastings, who is board-certified in Personal Injury Trial Law, our firm prepares every case with the expectation of going to trial. As a Texas infant intubation injury lawyer team, we investigate neonatal cases by reconstructing the clinical timeline and consulting with nationally recognized neonatal experts.
There is no cost for a free case review, and we do not collect attorney fees unless we secure a recovery for your family. If you have questions about your child’s care, contact Hastings Law Firm to speak with our team and take the first step toward answers.
Frequently Asked Questions About Infant Intubation Injury in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
