

Texas Infant Compartment Syndrome Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Infant compartment syndrome is a time sensitive emergency where rising pressure in a limb can cut off blood flow and cause rapid tissue damage. Because babies cannot describe pain, warning signs can be missed or dismissed, and delays in testing or treatment can lead to permanent nerve injury, scarring, disability, amputation, or worse. The condition is often linked to issues such as IV infiltration or overly tight casting, and prompt decompression surgery may be required. If you or a loved one were harmed or worse due to infant compartment syndrome in Texas, contact Hastings Law Firm for a free, confidential case review.
Top Rated Texas Medical Attorneys for Infant Injuries
What You Should Know About Neonatal Pressure Necrosis Claims in Texas:
- Permanent disability can result when infant compartment syndrome is not treated quickly because prolonged loss of blood flow can cause irreversible muscle and nerve damage.
- Amputation can become necessary when pressure related tissue injury progresses to severe tissue decay.
- Fatal outcomes can occur when compartment syndrome leads to systemic infection or sepsis.
- Preventable harm can follow delayed recognition in infants because they cannot self report pain and clinicians must rely on observable signs.
- Disputes often focus on whether warning signs were ignored or misattributed because swelling and skin color changes may be dismissed as normal recovery.
- Liability can extend beyond a single physician because nurses, surgeons, and hospitals may share responsibility based on their roles and documentation.
- Options in Texas can be limited by procedural requirements because medical malpractice claims require an expert report and other mandated steps.
- Recovery for non economic harm in Texas can be restricted because state law caps non economic damages while allowing economic damages.
- Long term financial burden can be substantial because future medical care, therapy, assistive devices, and accommodations may be needed for life.
- Medical records can be central to what happened because nursing notes, IV logs, and physician orders may show delays in monitoring, testing, or escalation.

A Healthcare Focused Law Firm
When your child suffers an injury that you believe could have been prevented, the weight of that realization is difficult to describe. You may feel certain something went wrong, yet unsure how to prove it or where to turn. That confusion is completely understandable, and you are not alone in feeling it.
Compartment syndrome in infants is a serious, time-sensitive condition. Founded by board-certified trial attorney Tommy Hastings in 2005, Hastings Law Firm focuses exclusively on medical malpractice cases. Our team of attorneys, in-house nurse consultants, and former defense attorneys investigates these cases from day one with one goal: finding out what happened and holding the responsible parties accountable.
If your child was harmed by a delayed or missed diagnosis, we can review the medical records and explain your legal options. The consultation is free and confidential.
Understanding Infant Compartment Syndrome and Neonatal Pressure Necrosis
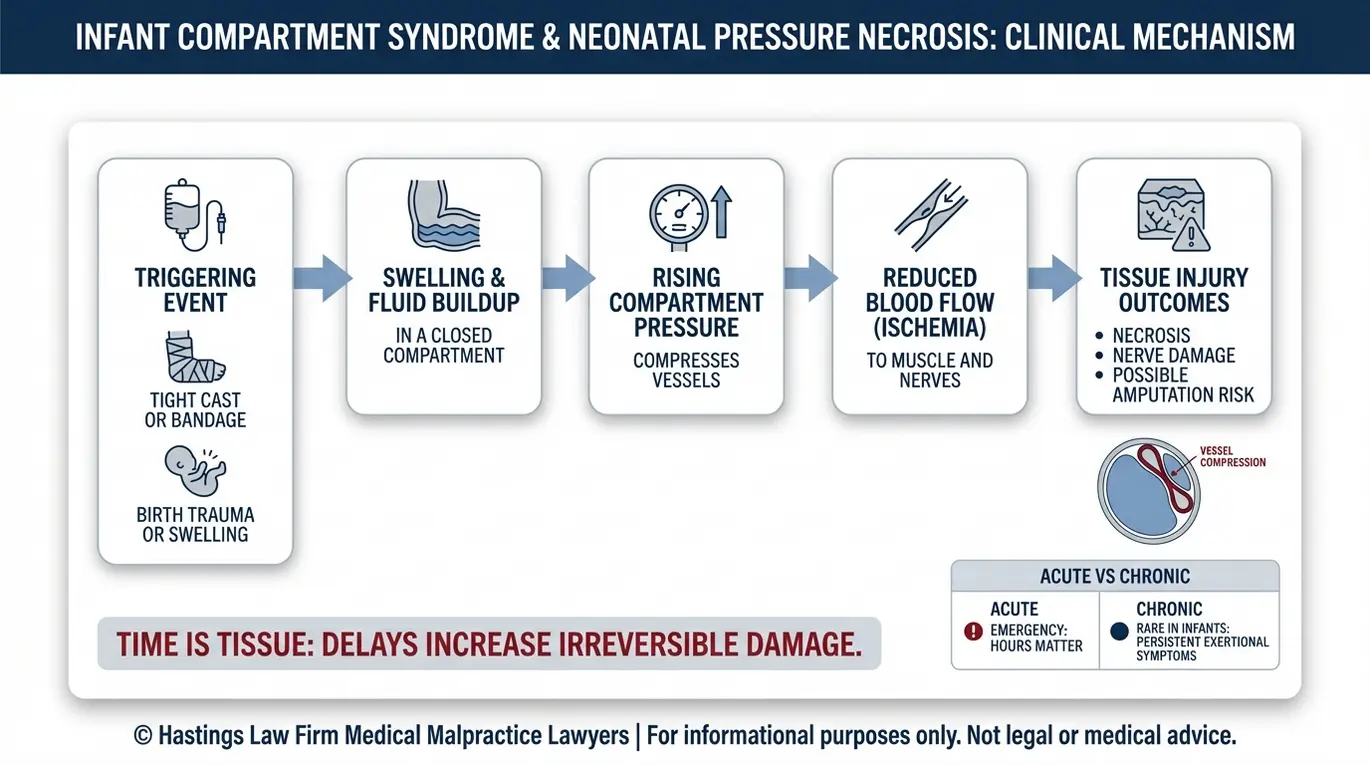
Infant compartment syndrome occurs when excessive pressure builds within a specific muscle group, restricting blood flow and causing rapid tissue death or neonatal pressure necrosis. Neonatal pressure necrosis refers to tissue death in newborns caused by external force or internal swelling, and it can progress quickly to irreversible harm if not treated promptly.
To understand why this condition is so dangerous, it helps to understand the basic mechanism. Muscles in the arms and legs are surrounded by a tough membrane called fascia. When swelling or bleeding occurs inside one of these enclosed spaces, pressure rises. That elevated pressure compresses blood vessels, cutting off circulation, a condition known as ischemia.
Without adequate blood flow, muscle tissue begins to die. In infants, whose tissues are especially fragile, this process can accelerate rapidly. Several factors can trigger dangerous pressure buildup in a newborn or infant:
- IV infiltration (extravasation injury): This occurs when intravenous fluid or medication leaks out of the vein and into the surrounding tissue. According to a case series published in PubMed Central on neonatal extravasation injuries, early identification is critical because the leaked fluid can cause significant swelling and compartment pressure in a very small limb.
- Tight casting or bandaging: Casts or wraps applied to treat fractures or congenital conditions like clubfoot can become dangerously constrictive as the limb swells.
- Birth trauma: Difficult deliveries, prolonged labor, or improper positioning can cause internal bleeding or swelling that leads to compartment pressure.
- Post-surgical swelling: Procedures on infant limbs, particularly orthopedic surgeries, carry a risk of swelling that must be closely monitored.
Acute compartment syndrome is a medical emergency requiring immediate intervention, while chronic compartment syndrome develops gradually over time. In infants, the concern is almost always acute. The window for effective treatment is measured in hours, not days.
Texas infant compartment syndrome attorneys evaluate these cases by reconstructing the clinical timeline, examining nursing notes, IV logs, and physician orders to determine whether the standard of care was met.
Improper Casting or Immobilization as a Cause of Injury
Routine procedures like casting for clubfoot correction or fracture management can become dangerous when applied incorrectly to an infant. A circumferential cast, one that wraps entirely around the limb, creates a rigid enclosure. If the limb swells after application, the cast does not expand with it. Pressure builds inside the enclosed space, and without intervention, blood flow is compromised.
The standard of care typically requires an orthopedic surgeon or treating provider to account for expected post-procedure swelling. One standard precaution is cast bivalving, which involves cutting the cast along both sides to allow the limb room to expand safely. When providers fail to anticipate swelling or neglect to check circulation after casting, a treatable situation can become a permanent injury.
Recognizing Critical Symptoms in Infants Unable to Communicate
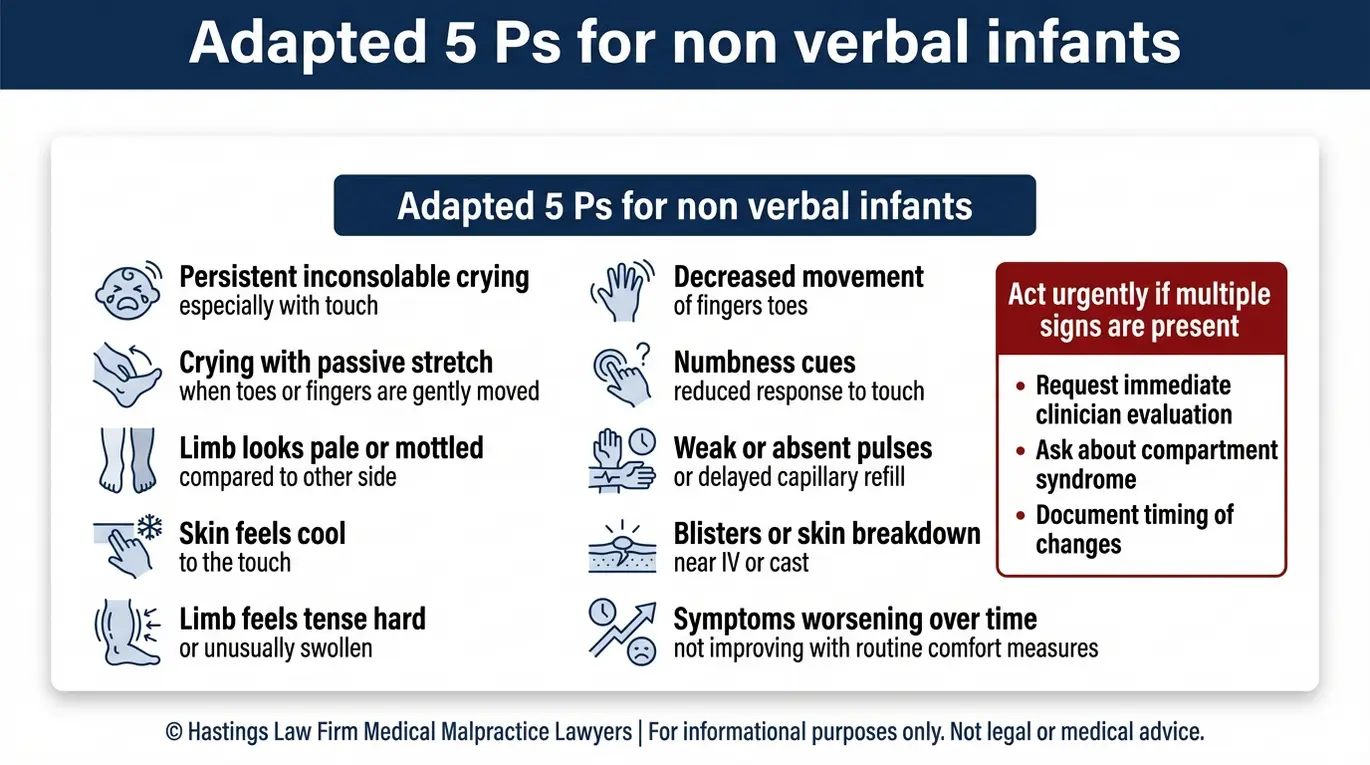
Because infants cannot verbalize pain, caregivers and medical staff must rely on observable signs such as persistent crying, skin that is cool to the touch, unnatural paleness, or a limb that feels tense and swollen. Recognizing these symptoms early is essential, and the burden falls almost entirely on the adults providing care.
In older children and adults, clinicians use a framework called the “5 Ps” of compartment syndrome to guide diagnosis. These five warning signs are Pain, Pallor (pale or discolored skin), Paresthesia (numbness or tingling), Pulselessness (loss of a detectable pulse in the affected limb), and Paralysis (inability to move the limb). Each indicator points to worsening pressure and declining circulation.
This framework was designed for patients who can describe what they feel. A baby cannot report numbness. A newborn cannot say the pain feels out of proportion to the injury, which is one of the earliest and most telling clinical signs.
As a result, a research article on acute compartment syndrome in children published in PubMed Central warns clinicians to “beware of silent compartment syndrome” in patients who cannot self-report. This places a higher responsibility on medical staff to be proactive.
One clinical technique used to assess pain in non-verbal patients is the passive stretch test. This involves gently extending the fingers or toes of the affected limb. If the infant reacts with intense, disproportionate crying during passive movement, it can suggest rising compartment pressure.
The table below adapts the standard 5 Ps framework to observable signs in infants:
| Clinical Sign | Adult Presentation | Infant Equivalent |
|---|---|---|
| Pain | Reports pain “out of proportion” | Inconsolable crying, especially with passive stretch of fingers or toes |
| Pallor | Skin appears pale or dusky | Limb appears white, blue, or mottled compared to unaffected limb |
| Paresthesia | Reports tingling or numbness | Decreased response to touch on the affected limb |
| Pulselessness | Weak or absent pulse | Weak or absent pulse detected by Doppler or palpation |
| Paralysis | Cannot move the limb | No spontaneous movement of the affected limb; limp or rigid posture |
When any combination of these signs appears, medical staff have a duty to act quickly. Waiting for all five to present before escalating care can mean the difference between a full recovery and permanent damage.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

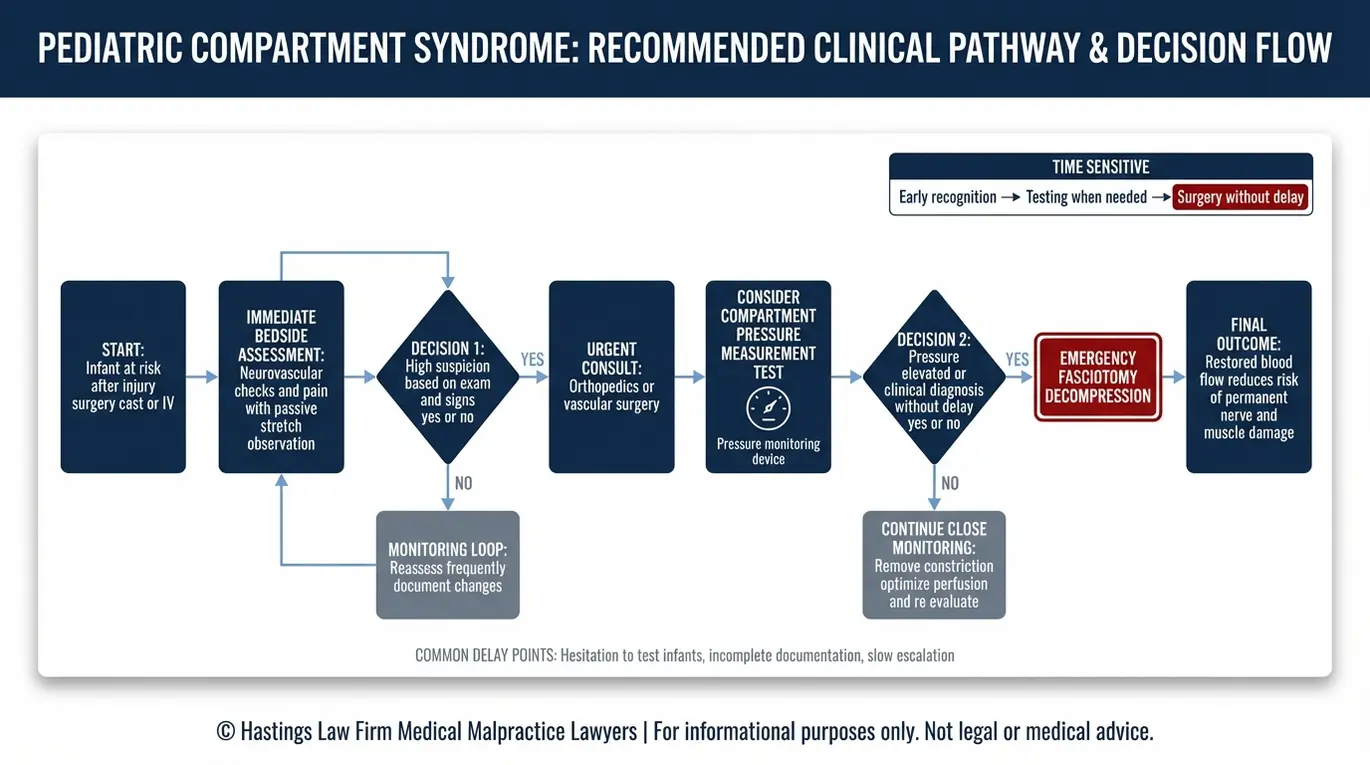
Diagnosing and Treating Compartment Syndrome in Pediatric Patients
Diagnosis requires clinical observation and a compartment pressure measurement test, followed immediately by a fasciotomy to release pressure and restore blood flow before permanent damage occurs.
The primary diagnostic tool is a device called a Stryker needle. This is a pressure monitoring device inserted into the muscle compartment to measure the internal pressure. Normal compartment pressure is low. When the measured pressure approaches or exceeds the threshold relative to the patient’s blood pressure, emergency fasciotomy becomes urgent.
Clinicians sometimes hesitate to perform this test on infants. The needle insertion is invasive, and the small size of an infant’s limb can make the procedure technically challenging. That hesitation can be costly.
According to the NCBI Bookshelf overview on acute compartment syndrome in children, clinical suspicion alone may justify treatment when the presentation is consistent, particularly in patients who cannot communicate their symptoms.
The only definitive treatment for compartment syndrome is a fasciotomy, sometimes called decompression surgery. During this procedure, a surgeon cuts open the fascia surrounding the affected muscle compartment, immediately relieving the trapped pressure and allowing blood flow to return. This may involve an orthopedic surgeon, a vascular surgeon, or both, depending on the location and severity of the injury.
The clinical reality is straightforward: time is tissue. Every hour that passes without decompression increases the risk of irreversible muscle death, nerve damage, and ultimately amputation. The standard sequence in a properly managed case generally follows these steps:
- Clinical suspicion identified: Provider observes signs consistent with rising compartment pressure (swelling, pain response, skin changes).
- Pressure measurement performed: Stryker needle or similar device confirms elevated compartment pressure.
- Surgical team mobilized: Orthopedic or vascular surgery is consulted immediately.
- Fasciotomy performed: Surgical decompression is completed as an emergency procedure.
- Post-operative monitoring: The limb is monitored for restored circulation, and additional surgeries may be needed for wound closure.
When any step in this sequence is delayed or skipped, the infant’s prognosis changes dramatically. Our legal and medical team examines each phase of this timeline to identify where breakdowns occurred and whether the standard of care was met.
When Does Failure to Diagnose Constitute Medical Malpractice
Medical malpractice occurs when a healthcare provider deviates from the accepted standard of care by ignoring clear symptoms or delaying necessary testing, and that deviation directly results in permanent injury or worsening necrosis.
The standard of care refers to the level of treatment a reasonably competent medical professional would provide under similar circumstances. For infants at risk of compartment syndrome, this standard generally includes frequent neurovascular checks, monitoring for swelling, and prompt diagnostic testing when warning signs appear. This applies specifically to infants recovering from orthopedic surgery, IV placement, or casting.
A failure to diagnose claim does not require proving that the doctor acted with bad intentions. It requires showing that the provider failed to do what other qualified professionals in the same specialty would have done, and that this failure caused harm. A misdiagnosis, such as attributing compartment syndrome symptoms to normal post-surgical swelling, can form the basis of a claim if a competent provider would have recognized the difference.
The concept of failure to rescue is often central to these claims. This refers to a situation where a provider identifies a complication, such as rising compartment pressure, but fails to act with the necessary speed or effectiveness to prevent harm. When a hospital’s system allows a patient to deteriorate despite clear warning signs, the institution itself may be liable for failing to enforce safety protocols.
Examples of conduct that may constitute negligence in these cases include:
- Dismissing persistent swelling or skin color changes as “normal”
- Failing to order a compartment pressure measurement when clinical signs were present
- Delaying surgical consultation after abnormal pressure readings
- Not monitoring an infant’s limb circulation after casting or IV placement
- Ignoring parental reports of their baby’s unusual distress or crying
Liability in these cases can extend beyond the individual physician. Nurses, surgeons, and the hospital as an entity may each bear responsibility depending on their role and what the records show.
Under the Texas Civil Practice and Remedies Code, Chapter 74, medical malpractice claims in Texas require specific procedural steps, including an expert report filed within 120 days of the defendant’s original answer. Working with a Texas infant compartment syndrome lawyer experienced in these requirements is essential to building a viable case.
Nursing Escalation and Advocacy Duties
Nurses are often the first to observe changes in an infant’s condition. They check vitals, assess limb circulation, and document clinical findings throughout their shift. When a nurse identifies signs of deterioration, the standard of care requires them to escalate those concerns through the chain of command.
If a surgeon dismisses a nurse’s report of increased swelling or changes in skin color, the nurse has a professional and legal duty to continue advocating. This includes contacting a charge nurse, nursing supervisor, or the hospital’s rapid response team. A failure to escalate can itself constitute negligence, and the hospital may be held liable for systemic failures in its hospital protocols.
Long Term Complications and Damages From Delayed Treatment
Complications from untreated compartment syndrome range from permanent nerve damage and foot drop to gangrene requiring amputation, resulting in lifelong medical needs and disability.
When blood flow is cut off for too long, muscle and nerve tissue die. One of the most well-documented consequences is Volkmann’s contracture, a permanent shortening and tightening of the forearm or leg muscles caused by prolonged ischemia. This deformity occurs when the necrotic muscle tissue is replaced by fibrous scar tissue, which is inelastic and shortens the muscle length.
As the scar tissue matures, it pulls the joint into a fixed position, often requiring multiple release surgeries to restore even partial range of motion. Other physical outcomes include foot drop, the inability to lift the front of the foot due to nerve damage. Chronic pain, loss of sensation, and in the most severe cases, gangrene, the death and decay of tissue that often requires partial or full amputation, can also occur.
Neonatal pressure necrosis can leave visible scarring and functional limitations that persist into adulthood. If compartment syndrome progresses to systemic infection or sepsis, the outcome can be fatal, giving rise to a wrongful death claim on behalf of the family.
The financial burden of these injuries extends over a lifetime:
| Injury | Potential Long-Term Costs |
|---|---|
| Nerve damage / Foot drop | Ongoing physical therapy, orthotics, adaptive equipment |
| Volkmann’s contracture | Reconstructive surgeries, occupational therapy, assistive devices |
| Amputation | Prosthetics (replaced multiple times as the child grows), rehabilitation, home modifications |
| Chronic pain / Disability | Pain management, mental health treatment, reduced future earning capacity |
| Wrongful death | Funeral expenses, loss of companionship, loss of the child’s future earning potential |
In medical malpractice cases involving children, damages for future medical expenses, custodial care, and lost earning capacity can be substantial because they account for an entire lifetime of need. Costs for these injuries are not limited to childhood. A child with severe nerve damage may require adaptive housing, modified vehicles, and vocational training well into adulthood.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
Compartment syndrome injuries in infants are often preventable. When medical professionals fail to monitor, diagnose, or treat this condition in time, families deserve to know what happened and why.
At Hastings Law Firm, we prepare every case as if it will go to trial. Our team includes in-house nurses, former defense attorneys, and a national network of medical experts who understand how to identify breakdowns in care and prove them. As a Texas infant compartment syndrome law firm, we handle these cases on a contingency fee basis, meaning you pay no attorney fees or costs unless we secure a recovery for your family.
If your child suffered a preventable injury, contact our team today for a free, confidential case evaluation. We will review the medical records, consult with the right experts, and give you honest answers about your options.
Call Hastings Law Firm or reach out online to schedule your free consultation.
Frequently Asked Questions About Infant Compartment Syndrome in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
