

Arizona Informed Consent Interpreter Failure Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Non English speaking patients can be seriously harmed when a hospital fails to provide a qualified medical interpreter during informed consent. Without clear communication about risks, benefits, and alternatives, a signed consent form may not reflect real understanding. The article describes how ad hoc interpreters and remote interpreting failures can distort critical information, and how Arizona and federal standards treat language access as a patient safety requirement. It also explains how hospitals may face direct responsibility for systemic language access breakdowns. If you or a loved one were harmed or worse due to informed consent interpreter failure in Arizona, contact Hastings Law Firm for a free, confidential case review.
Top-Rated Legal Representation for Non-English Speaking Patients in Arizona
What You Should Know About Non-English Speaking Patient Negligence Claims in Arizona:
- Serious medical injury can result when informed consent occurs without communication in a language the patient understands.
- Options can expand when a signed consent form carries little weight because there was no meaningful comprehension of what was agreed to.
- Liability can extend beyond an individual clinician when a hospital fails to create or enforce language access protocols.
- Recovery can be affected when a hospital relies on an emergency implied consent justification that does not fit the actual circumstances.
- Patient safety can be undermined when ad hoc interpreters such as family members or untrained staff translate complex medical information.
- Harm can follow when interpreter errors change the meaning of key details such as allergies or medication instructions.
- Communication can break down even with professional services when remote interpreting has poor audio or video quality.
- Disputes can turn on what the medical record shows about interpreter use because missing documentation may indicate language access was not provided.

A Healthcare Focused Law Firm
Every patient has the right to understand what a doctor is proposing before agreeing to a medical procedure. When a hospital fails to provide a qualified interpreter, that right is taken away, and the consequences can be devastating. For patients with limited English proficiency, a language barrier during the consent process is not just an inconvenience; it can be the direct cause of a serious medical injury.
If you or a loved one was harmed after a healthcare provider failed to communicate in a language you understand, you may have a valid medical malpractice claim. As an Arizona Informed Consent Interpreter Failure Lawyer, Hastings Law Firm focuses exclusively on medical negligence cases like these. Our team includes in-house medical professionals who know how to identify where the system broke down. Contact us for a free, confidential case evaluation to learn what your options are.
Informed Consent Laws in Arizona and Rights for Non-English Speakers
Informed consent requires that a patient genuinely understands the risks, benefits, and alternatives of a proposed treatment before agreeing to it. In Arizona, if a healthcare provider fails to communicate this information in a language the patient understands, either directly or through a qualified interpreter, the consent may be invalid, and the provider can be held liable for medical negligence.
Informed consent is not just a form to sign. It is a process, a conversation between doctor and patient where the provider explains what will happen, what could go wrong, and what other options exist. Legally, performing a procedure without valid consent can be considered battery, an unauthorized touching of the patient. Because the patient did not understand the nature of the act due to the language barrier, they effectively did not consent to it at all.
The law recognizes that the right to determine what happens to one’s own body is a top priority, and language barriers do not forfeit this right. The patient must have the opportunity to ask questions and receive answers they can actually comprehend. When the patient speaks limited or no English, that process demands qualified language assistance.
Federal law reinforces this standard. Title VI of the Civil Rights Act of 1964 prohibits discrimination based on national origin in any program receiving federal funding, which includes virtually every hospital and clinic that accepts Medicare or Medicaid. Compliance requires more than just hiring a bilingual staff member; it mandates a systemic approach to language access that ensures competency and confidentiality. These statutes ensure that no person is denied the benefits of a federally assisted program simply because they cannot speak English.
Section 1557 of the Affordable Care Act strengthened these protections by requiring meaningful access to healthcare services for individuals with Limited English Proficiency (LEP). The federal government uses this term to describe anyone who does not speak English as their primary language or has a limited ability to read, write, speak, or understand English. The U.S. Department of Health and Human Services provides detailed guidance on these obligations.
These are not suggestions. They are legal mandates that establish a duty of care hospitals owe to every patient, regardless of the language they speak. A provider who skips the interpreter and hands a Spanish-speaking patient an English-only consent form has not met the standard of care. They have bypassed it entirely.
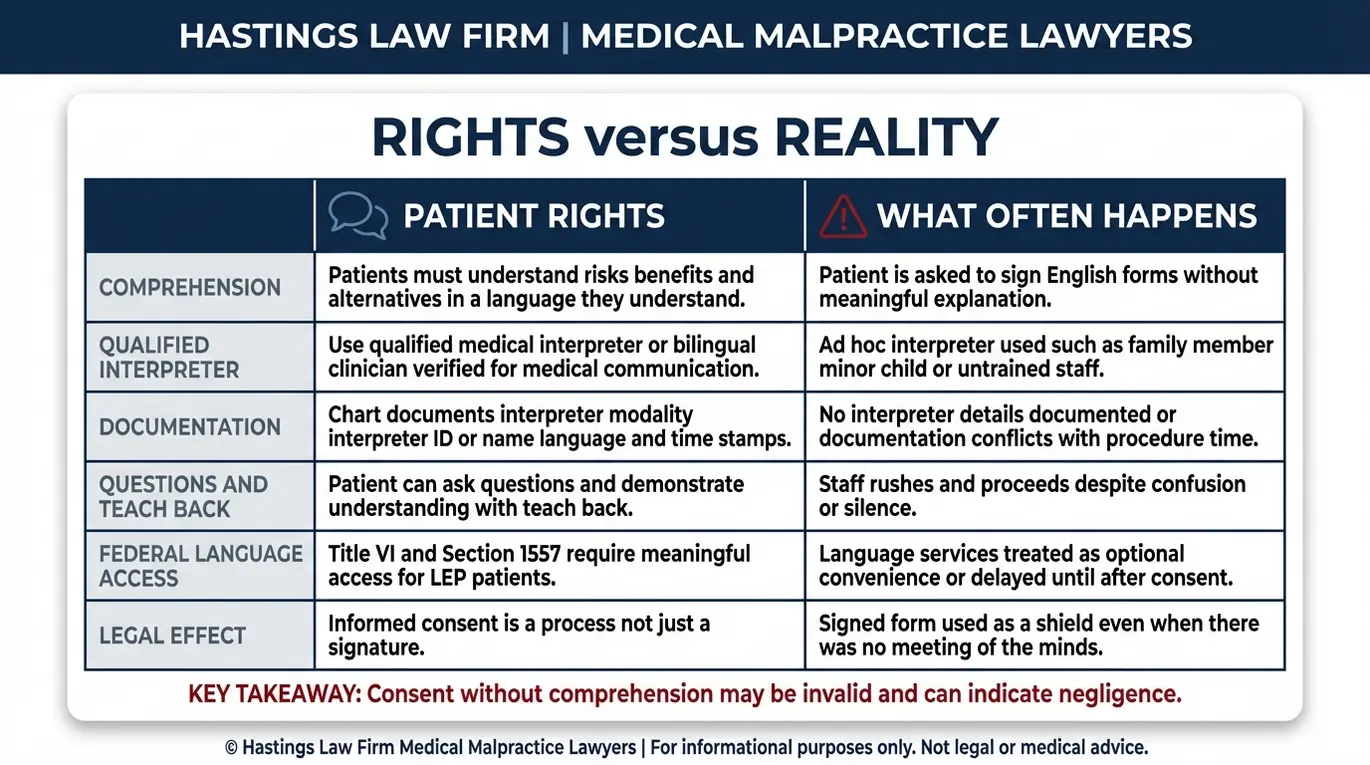
The gap between legal requirements and actual practice is often the starting point for these cases. This disparity highlights the negligence inherent in prioritizing speed over patient safety.
| What the Law Requires | What Often Happens |
|---|---|
| Qualified medical interpreter provided at no cost to the patient | Patient is handed forms in English with no interpreter present |
| Risks, benefits, and alternatives explained in the patient’s primary language | Medical staff assumes the patient “understands enough” English |
| Patient given time to ask questions and receive translated answers | Consent form is signed quickly before the patient can object |
| Interpreter must be trained in medical terminology and ethics | A family member, minor child, or bilingual janitor is asked to translate |
| Language access documented in the medical record | No record of interpreter services appears in the chart |
When a hospital treats the consent form as a checkbox rather than a meaningful exchange of information, patients with limited English proficiency are the ones who pay the price.
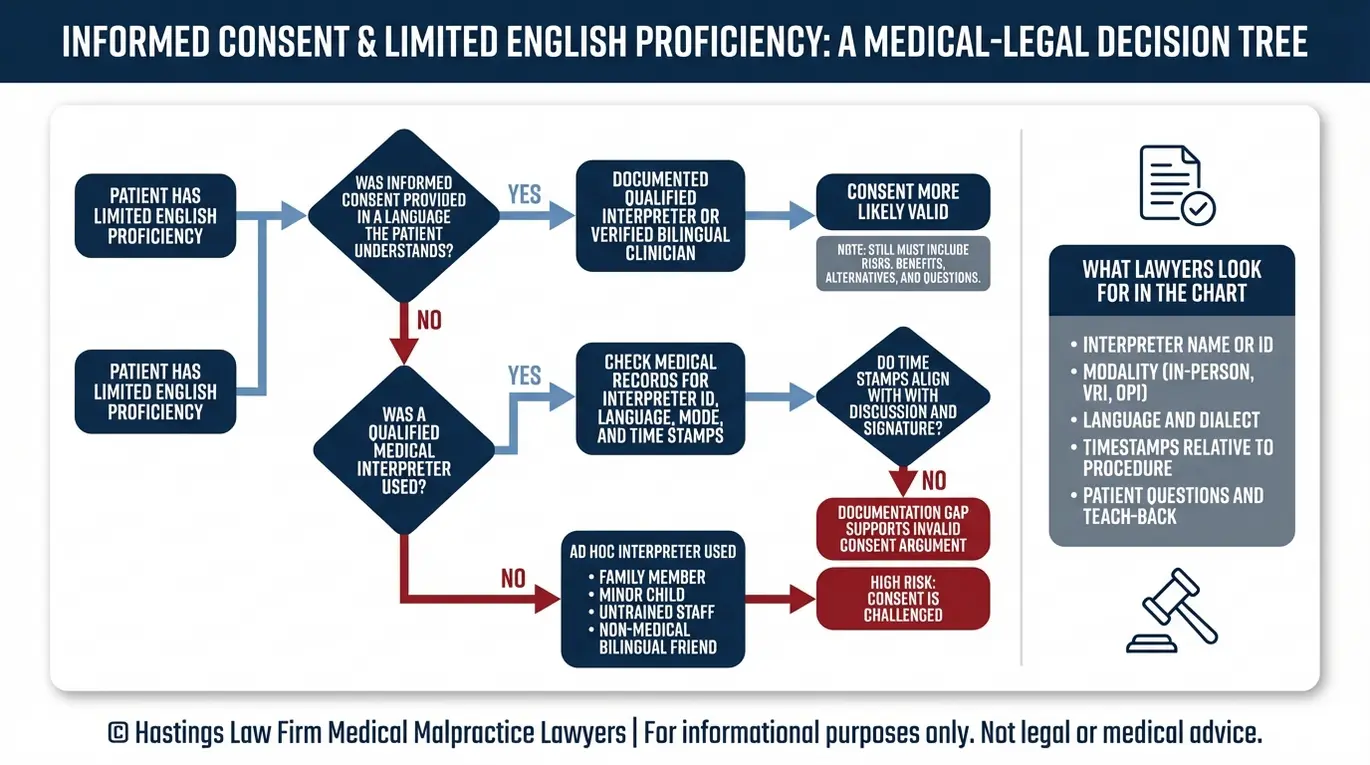
How Interpreter Failure Nullifies Medical Consent Forms
A signed consent form is not a defense if the patient could not read or understand it. Courts evaluate whether there was a true “meeting of the minds” between the physician and the patient. If the patient had no meaningful comprehension of what they were agreeing to, that signature may carry little to no legal weight in litigation.
Hospitals and their defense attorneys frequently point to the signed form as proof that the patient consented. But the form itself is only evidence that a pen touched paper. It says nothing about whether the patient understood the words printed on it. When we review these cases, we look at what actually happened in the room: who explained the procedure, in what language, and whether any interpretation was provided.
One of the most common failures involves the use of an ad hoc interpreter, meaning someone who is not a trained, certified medical interpreter but is pulled in as a substitute. This can include:
- A minor child asked to translate complex surgical risks for a parent
- A family member who may soften or censor difficult medical information
- A bilingual janitor, receptionist, or other untrained staff member
- A friend or fellow patient in the waiting room
These individuals are not qualified to handle the precision required in medical communication. A certified medical interpreter is someone who has been professionally trained and tested in medical terminology, ethical standards, and accuracy protocols. The difference between the two can be the difference between a patient understanding “there is a risk of paralysis” and a family member saying “they said it should be fine.”
The National Standards for Medical Interpreters, published through the Commonwealth Fund, outline the training, competency, and ethical requirements that define qualified interpretation in healthcare. When hospitals ignore these standards, the consent process collapses.
In contract law and medical jurisprudence, a “meeting of the minds” implies that both parties understood the terms of the agreement. Without this mutual understanding, the medical consent is voidable. Defense counsel will argue the signature is binding, but we demonstrate that the signature was obtained through a fundamental failure of communication, rendering the document legally hollow.
Consulting an Arizona Informed Consent Interpreter Failure Lawyer is essential when hospitals rely on signed forms despite language barriers. At Hastings Law Firm, our in-house medical staff and former defense attorneys know exactly how to challenge the validity of these forms. We examine the medical records for interpreter documentation, cross-reference procedure timestamps, and work with qualified experts to demonstrate that no real consent was ever given.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Common Interpreter Errors Leading to Medical Injury
Interpreter errors in medical settings generally fall into three categories: omissions—leaving out critical information; additions—inserting opinions the doctor never stated; and substitutions—mistranslating medical terms into something with a different clinical meaning. Any one of these errors can lead to misdiagnosis, surgical mistakes, or dangerous medication dosing when the patient cannot accurately describe symptoms or understand a provider’s instructions.
These are not hypothetical problems. One frequently cited case involved the Spanish word “intoxicado” being interpreted as “intoxicated” rather than its actual meaning, which is closer to “nauseated” or “poisoned.” That single mistranslation led to a misdiagnosis and a delayed treatment that caused lasting harm. Errors like these happen when untrained individuals are placed in a role that requires precise medical vocabulary.
| Error Type | Clinical Example | Potential Injury |
|---|---|---|
| Omission | Interpreter fails to translate a known drug allergy or listed side effect | Allergic reaction, anaphylaxis, or adverse drug interaction |
| Addition | Interpreter tells the patient “the doctor says it’s not serious” when the doctor made no such statement | Patient declines follow-up care or ignores warning signs |
| Substitution | “Kidney” is translated as “liver,” or “twice daily” becomes “twice weekly” | Wrong organ treated, medication underdosed or overdosed |
There is also the problem of interpreter neutrality. When an ad hoc interpreter, such as a family member, answers questions on behalf of the patient rather than translating the patient’s own words, the doctor loses access to the patient’s actual symptoms and concerns. The physician may then make clinical decisions based on incomplete or inaccurate information, and the patient has no idea the communication was compromised.
The Dangers of Telephonic and Video Interpretation Failures
Even when hospitals do arrange for professional interpretation, the method of delivery matters. Video Remote Interpreting (VRI), which uses a video screen to connect a remote interpreter, and Over-the-Phone Interpreting (OPI), which provides audio-only interpretation via telephone, are increasingly common in hospitals looking to reduce costs. While both can be effective when properly implemented, they carry real limitations.
Connection drops, poor audio quality, and background noise can all cause the interpreter to miss words or ask for repeated information during time-sensitive conversations. With OPI, the interpreter cannot see the patient at all, meaning visual cues like facial expressions, gestures indicating pain, or signs of confusion go unnoticed. VRI can have similar problems when the screen is poorly positioned or the video quality is low.
Federal regulations implementing Section 1557 of the Affordable Care Act set specific standards for how healthcare organizations must deliver remote language services. These regulations specifically require that if remote interpreting is used, the technology must produce high-quality audio and video that allows for effective communication. When a hospital cuts corners with cheap equipment or low-bandwidth connections, they are violating these federal standards and endangering patients. Facilities that rely on remote interpretation without ensuring quality and reliability may still fall short of their legal obligations, creating potential liability when communication failures contribute to a medical injury.
Exceptions and Emergency Consent in Arizona Law
Arizona law relies on implied consent, a legal doctrine allowing treatment in genuine emergency situations where a patient is incapacitated, facing an immediate threat to life or limb, and no surrogate decision-maker is available. Under these narrow circumstances, a provider may proceed without standard informed consent. However, this exception does not apply to scheduled surgeries, non-emergent stages of labor and delivery, or routine treatments where there was time to arrange an interpreter.
Emergency implied consent exists because the law does not require doctors to stand by while a patient dies simply because a form has not been signed. But the exception is designed to be narrow. It covers situations like an unconscious car accident patient arriving in the emergency department, not a pre-planned knee replacement where the hospital had days or weeks to arrange language services.
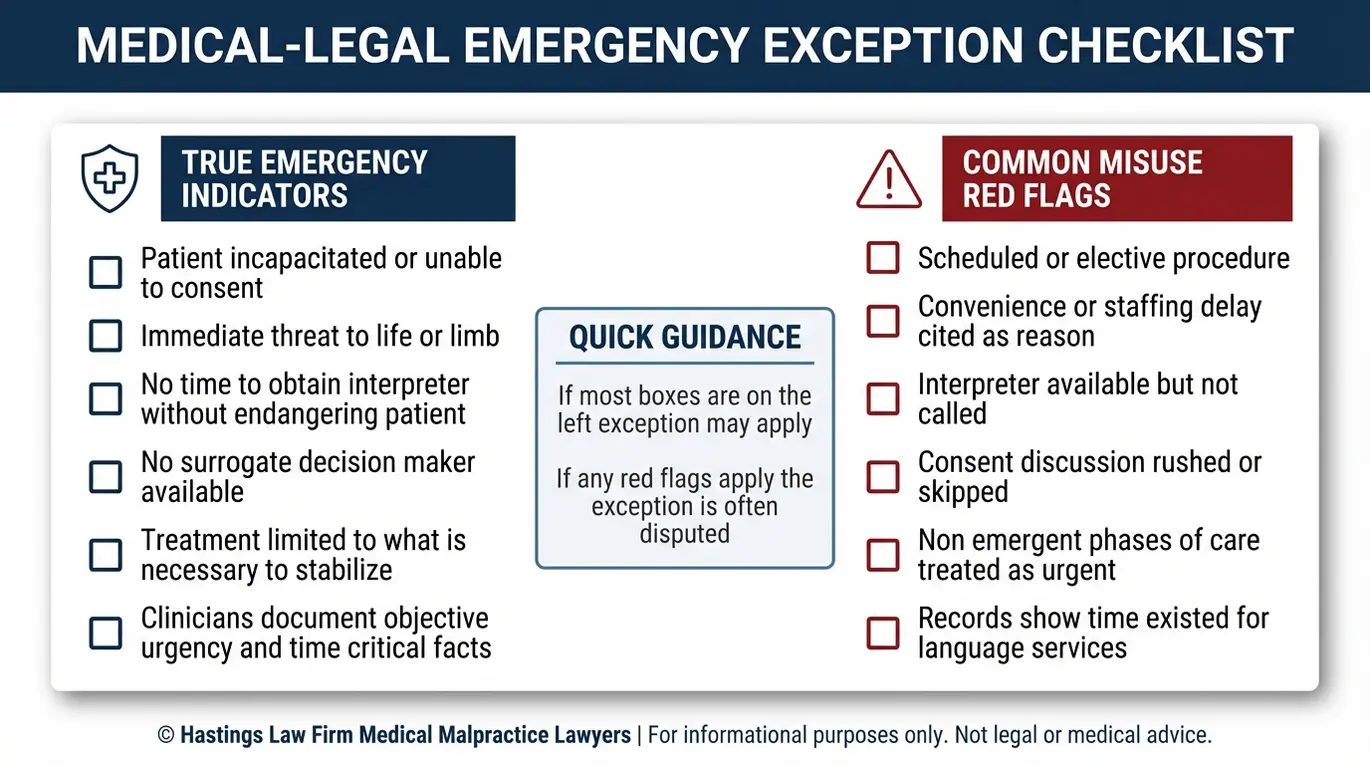
Hospitals sometimes invoke the emergency defense broadly, arguing that clinical urgency justified skipping the interpreter. We examine whether that characterization is accurate. The following checklist reflects what courts and investigators typically evaluate when determining if the emergency exception was properly applied:
- Was the patient unconscious or otherwise unable to communicate?
- Was there an immediate, life-threatening condition requiring instant intervention?
- Was there a surrogate decision-maker (spouse, parent, legal guardian) who could have been contacted?
- Did the facility have any advance notice of the procedure, such as a scheduled surgery or planned admission?
- Was there any window of time, even 15 or 30 minutes, where an interpreter could have been reached by phone or video?
- Did the medical record document why emergency consent was invoked instead of standard consent?
Hospitals often attempt to stretch the definition of “emergency” to cover situations where they simply failed to plan ahead. However, Arizona courts distinguish between a medical crisis and a scheduling error. If the patient was stable enough to wait for a specialist or a scan, they were stable enough to wait for an interpreter.
If the answer to most of these questions suggests that time and resources existed to use interpretation, the emergency defense weakens significantly. Waiting for an interpreter is not a medical emergency. It is a logistical responsibility.
At Hastings Law Firm, we build a detailed timeline of the events surrounding consent. Our team reviews admission records, nursing notes, and interpreter request logs to determine whether the facility genuinely had no opportunity to provide language access, or whether it simply did not try.
Establishing Corporate Liability for Language Access Violations
Liability for interpreter failure often reaches beyond the individual physician to the hospital or healthcare system itself. Under the theory of corporate negligence, a facility can be held directly liable if it fails to create, maintain, or enforce protocols for language access. This includes failing to contract with qualified interpreter services or failing to train staff on federal language access requirements. It also involves failing to implement a language access plan, which is a written policy that outlines how the facility identifies LEP patients and provides them with timely, competent interpretation.
The Culturally and Linguistically Appropriate Services (CLAS) Standards, published by the U.S. Department of Health and Human Services’ Office of Minority Health, provide the benchmark for what healthcare organizations should be doing. These standards call for interpreter services at all points of contact, staff training, and quality assurance measures. When a hospital has no such plan in place, or has a plan it does not follow, that gap becomes evidence of systemic negligence.
Federal enforcement actions reinforce this point. The Voluntary Resolution Agreement between the HHS Office for Civil Rights and Englewood Ear, Nose and Throat is one example where a facility was investigated and required to overhaul its language access practices after failing to provide adequate interpreter services. These Office for Civil Rights (OCR) resolutions can support a state-level negligence claim by establishing that the facility’s conduct fell below accepted standards.
Arizona’s medical malpractice statutes define the framework for these actions, including the elements a patient must prove. Under A.R.S. § 12-563, a plaintiff must establish that a health care provider failed to exercise the degree of care, skill, and learning expected of a reasonable, prudent provider, and that such failure was a proximate cause of the injury. When the breach is institutional, such as a hospital failing to provide interpreter services that its own policies require, vicarious liability may also apply.
Under vicarious liability, the hospital acts through its employees. This concept means the facility is responsible for the actions of its staff. If a nurse realizes a patient does not understand the English consent form but hands them a pen anyway, that nurse’s negligence is imputed to the hospital. The facility cannot hide behind the individual errors of its staff when those errors result from a lack of institutional oversight and training.
Our team at Hastings Law Firm examines facility policies, interpreter service contracts, staff training records, and OCR complaint history. We work with qualified experts to establish what the hospital’s obligations were and how its failures contributed to the patient’s injury. This approach allows us to identify every responsible party, not just the physician in the room.
Contact the Arizona Hospital Malpractice Attorneys at Hastings Law Firm Today for Help
Language access is not a courtesy. It is a patient safety requirement. When a hospital fails to provide a qualified interpreter, it strips patients of the ability to make informed decisions about their own medical care, and the consequences of that failure can change lives permanently.
If you or a loved one suffered a medical injury after a provider failed to communicate in your language, you deserve answers. As a dedicated Arizona Informed Consent Interpreter Failure Lawyer, Hastings Law Firm has the medical and legal team to investigate what happened. Our in-house nurses and board-certified patient advocates review your records, identify where protocols broke down, and work alongside our attorneys to build your case from day one.
We handle these cases on a contingency fee basis, meaning you pay no attorney fees or costs unless we recover compensation for you. Call us today or complete our online form for a free, confidential case evaluation. Let us help you understand what happened and what comes next.
Frequently Asked Questions About Informed Consent Interpreter Failure in Arizona

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
