

Texas High-Risk Pregnancy Transfer Failure Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
High risk pregnancy transfers can become emergencies when fetal distress is missed or a hospital handoff is delayed. Breakdowns in monitoring, communication, staffing, or transport coordination can leave a baby without timely intervention and can also put the mother at risk. Some injuries may not be obvious right away and can emerge later as developmental concerns. Texas law and damage limits can also affect what options remain after a suspected medical error. If you or a loved one were harmed or worse due to high risk pregnancy transfer failure in Texas, contact Hastings Law Firm for a free, confidential case review.

Top Rated High Risk Pregnancy Transfer Attorneys in Texas
What You Should Know About NICU Transfer Delay Claims in Texas:
- Permanent harm can result when an emergency transfer is delayed after fetal distress is missed or not escalated.
- Lasting effects may not be obvious at birth, since some birth injuries linked to oxygen deprivation can emerge later as missed developmental milestones.
- Options can narrow when transfer delays stem from communication gaps and administrative bottlenecks that are hard to reconstruct after the fact.
- Maternal outcomes can worsen when time sensitive complications are not recognized and acted on during labor.
- Accountability can extend beyond one clinician, since hospitals, birth centers, and transport teams may each contribute to a transfer chain breakdown.
- Additional injury can occur after arrival, since NICU delays in critical interventions can worsen outcomes.
- Catastrophic harm can be compounded by NICU medication dosing mistakes, including decimal errors that cause massive overdoses.
- Financial recovery can be limited for non economic losses in Texas, even when long term care needs are extensive.
- The ability to pursue a claim can be lost if filing deadlines are missed, including strict outer limits that can apply even when injuries are discovered later.
- Key records can be central to understanding what happened, including fetal monitoring strips, transfer logs, and medication administration documentation.

A Healthcare Focused Law Firm
When a high-risk pregnancy requires an emergency transfer and that transfer is delayed, the consequences for a mother and baby can be permanent. If your child suffered a birth injury that you believe was connected to a delayed or mismanaged hospital transfer, you deserve clear answers about what happened and why.
At Hastings Law Firm, our team focuses exclusively on medical negligence cases. Led by founder Tommy Hastings, a Board Certified trial lawyer with over 20 years of experience, our team includes in-house nurse consultants and board-certified patient advocates. As a Texas High-Risk Pregnancy Transfer Failure Lawyer, we understand the medical complexity behind these cases and the emotional weight families carry long after delivery. If something went wrong during your care, we can review your records and explain your legal options at no cost to you.
Failure to Detect Fetal Distress Requiring Emergency Transfer
A failure to detect fetal distress occurs when medical staff ignore or misinterpret electronic fetal monitoring data that indicates oxygen deprivation, delaying the necessary transfer to a facility equipped for emergency intervention.
During labor, a baby’s wellbeing is assessed primarily through continuous electronic fetal monitoring (EFM), a form of fetal heart rate monitoring that tracks the baby’s heart rate in relation to contractions. This data produces what is called a fetal heart rate tracing, which clinicians classify into three categories. Category I tracings are normal. Category II tracings are indeterminate and require close observation. Category III tracings are abnormal, signaling that the baby may not be getting enough oxygen and that immediate action is needed.
The standard of care requires that nurses, midwives, and obstetricians continuously evaluate these tracings and respond appropriately. According to the National Center for Biotechnology Information (NCBI Bookshelf), fetal heart rate classifications guide clinical decisions about when to intervene, including when to initiate an emergency transfer or cesarean delivery.
When fetal distress, a condition where the baby shows signs of inadequate oxygen supply, goes unrecognized or unaddressed, even a short delay can lead to serious harm. A Texas High-Risk Pregnancy Transfer Failure Lawyer knows that oxygen deprivation lasting only minutes can cause permanent brain damage.
Signs of fetal distress that should prompt immediate escalation include:
- Persistent late decelerations in the fetal heart rate after contractions
- Minimal or absent heart rate variability over an extended period
- Prolonged bradycardia (a sustained drop in the baby’s heart rate)
- Category III tracing patterns that do not improve with standard interventions
- Tachycardia combined with other concerning findings
Nurses and midwives are often the first to observe these warning signs. Their role in recognizing the need for escalation is critical. If a nurse identifies a Category III tracing and the attending physician does not respond, the standard of care may require the nurse to activate a chain-of-command protocol to get the baby delivered or transferred to a higher-level facility.
When oxygen deprivation persists, it can cause hypoxic-ischemic encephalopathy (HIE), a type of brain injury resulting from reduced blood flow and oxygen to the brain. A systematic review published in PubMed Central confirms the relationship between neonatal HIE and long-term cognitive impairment, including deficits in memory, attention, and learning.
Early Identification of Symptoms Emerging 12 to 24 Months Later
One of the most difficult aspects of birth injuries caused by transfer delays is that the damage may not be obvious at birth. These milestones are physical and cognitive markers that signal healthy growth. Hypoxic-ischemic encephalopathy (HIE), which is brain damage caused by oxygen deprivation during or around delivery, can take months to reveal its full impact.
Many parents first notice something is wrong when their child begins missing developmental milestones between 12 and 24 months of age. A baby who isn’t sitting, crawling, or babbling on schedule may later receive a diagnosis of cerebral palsy or another form of brain injury linked to the birth event.
This delayed presentation is one reason these cases are so often overlooked. The connection between a transfer delay at birth and a developmental diagnosis a year or two later is not always obvious to families. Our legal and medical team is experienced in tracing those connections back to the clinical timeline.

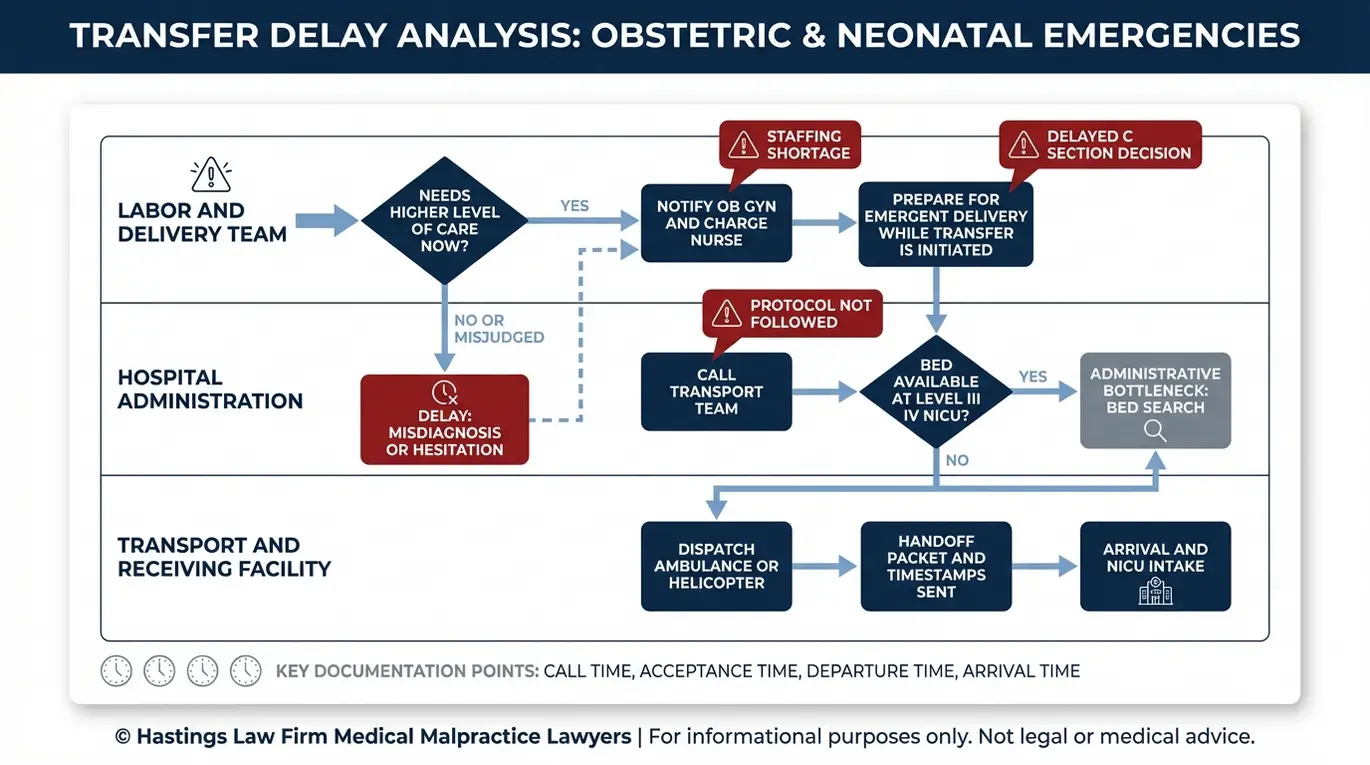
Common Causes of Transfer Delays in High Risk Pregnancies
Transfer delays are frequently caused by inadequate staffing, administrative bottlenecks, hesitation to perform C-sections due to legal ambiguity, or a failure to follow established emergency transport protocols. A high-risk pregnancy, one involving conditions such as preeclampsia, placental complications, or fetal growth restriction, demands a level of monitoring and readiness that not every facility can provide.
When a facility lacks the resources to manage an emerging crisis, the standard of care generally requires a timely transfer to a hospital with the appropriate level of care. Breakdowns can occur at several points along the way.
Administrative Failures
In some cases, the delay begins before a doctor ever makes the call. These failures often involve poor coordination between hospital departments. Transport teams may not be contacted promptly. Available beds at receiving hospitals may not be confirmed in time. Communication gaps between nursing staff, physicians, and dispatch can introduce dangerous delays that compound as minutes pass.
Medical Hesitation
Medical hesitation occurs when providers wait too long to act on clinical signs. An obstetrician (OB-GYN) or midwife may hesitate to escalate care or recommend an emergency cesarean (C-section) when the clinical picture is ambiguous. Misreading labor progression, underestimating the severity of a Category II fetal heart tracing, or waiting too long to intervene can result in a delayed C-section that might have prevented injury.
Obstetic Complications Requiring Immediate Transfer
Certain conditions demand access to a Level III or Level IV NICU that smaller hospitals and birth centers simply cannot provide. These include preeclampsia and HELLP syndrome (a severe variant involving liver and blood clotting dysfunction), umbilical cord complications such as prolapse or compression, and meconium-stained amniotic fluid, which is the presence of a baby’s first stool in the fluid surrounding it, indicating possible fetal distress.
| Cause of Delay | Potential Consequence |
|---|---|
| Delayed call to transport team | Extended oxygen deprivation during transit gap |
| Bed unavailability at receiving hospital | Forced diversion to less-equipped facility |
| Misinterpretation of fetal monitoring strips | Missed window for emergency C-section |
| Failure to recognize preeclampsia or HELLP syndrome | Maternal seizure, stroke, or organ damage |
| Meconium-stained fluid left unaddressed | Aspiration syndrome and respiratory failure in the newborn |
A Texas high-risk pregnancy transfer failure lawyer experienced in these cases knows that a delay of even 20 to 30 minutes can change the outcome entirely. Our investigation focuses on pinpointing where and why the breakdown occurred.
Impact of Texas Human Life Protection Act on Emergency Care
Recent legislative changes in Texas have created additional concerns around emergency obstetric care. Some OB-GYNs have expressed hesitation about performing certain emergency interventions, including procedures like dilation and curettage (D&C), out of concern about potential legal consequences under evolving state law.
When a provider hesitates to act in a genuine medical emergency, the result can be a delay that falls below the standard of care. Medical negligence is not defined by a provider’s motivation; it is defined by whether the care delivered met accepted medical standards. While Texas tort reform/damage caps limit financial recovery, the fear of criminal prosecution under new laws can impact the care provided during labor. If fear of legal repercussions contributed to a failure to perform an emergency cesarean section or other necessary intervention, the clinical outcome, not the reason for the hesitation, is what our investigation examines.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

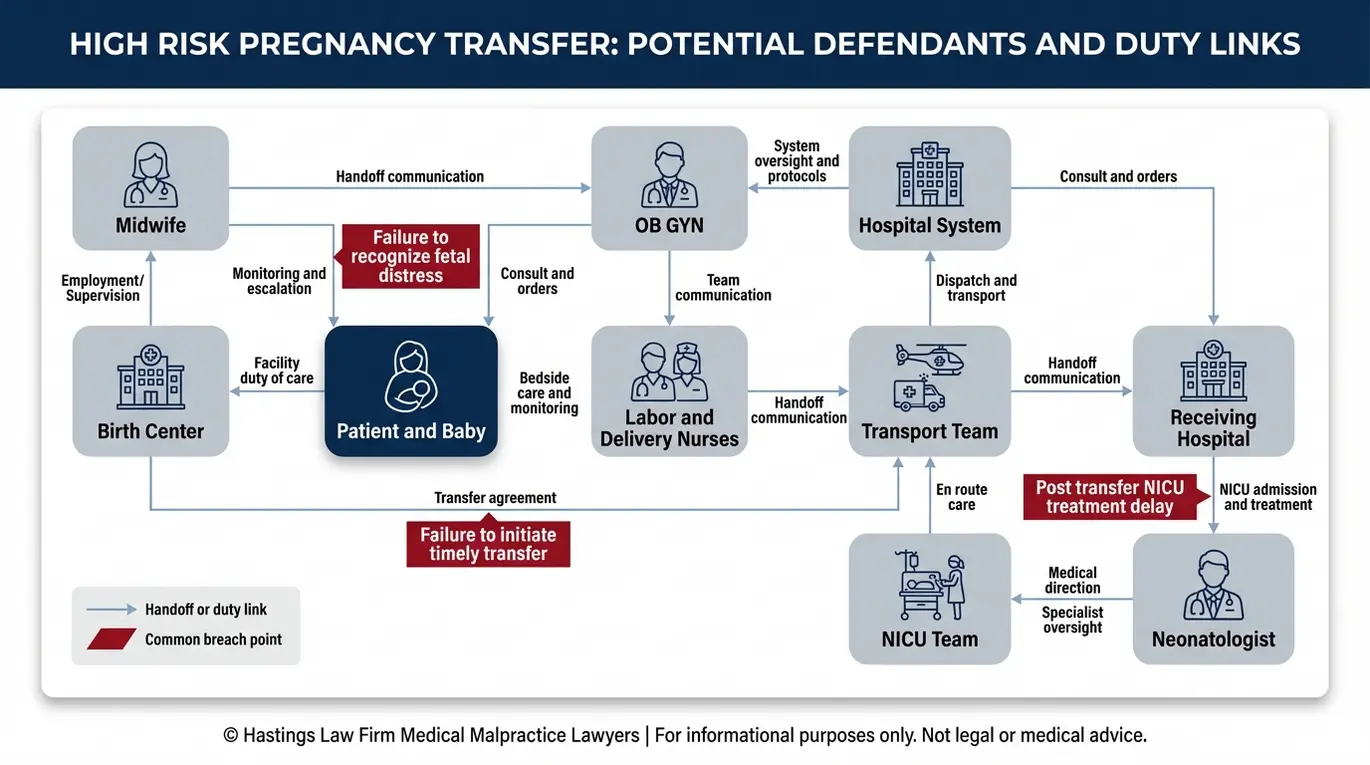
Liability in Transfer Failure Cases for Hospitals and Birth Centers
Liability can extend beyond the attending physician to include midwives, birth centers for violating transfer agreements, hospital systems for administrative failures, and transport teams for en-route negligence. Liability in these cases determines which parties are legally responsible for medical errors. Understanding who bears responsibility requires a careful review of every handoff, decision point, and transfer chain communication gap.
Hospital Systems
Hospital systems are responsible for the safety protocols that govern patient care. A hospital may be liable for institutional failures that contributed to the delay or the injury. This includes inadequate staffing levels, broken or unavailable equipment, and the absence of protocols for rapid response in obstetric emergencies. Research published in PubMed Central on interprofessional communication in obstetrics confirms that breakdowns in team communication are a leading contributor to preventable adverse events in labor and delivery settings.
NICU Negligence After Transfer
Liability does not end when the baby arrives at the receiving hospital. If the higher-level facility fails to provide timely and appropriate care, that institution and its staff can also be held accountable. Delays in initiating therapeutic hypothermia, commonly called cooling therapy (a treatment that lowers a newborn’s body temperature to reduce brain damage after oxygen deprivation), or failure to manage complications like sepsis can worsen outcomes significantly. Cooling therapy must typically begin within six hours of the injury to be effective.
A Level III neonatal intensive care unit (NICU) provides specialized care for seriously ill newborns, while a Level IV NICU offers the highest level of care, including surgical capabilities. If a baby is transferred to a facility that lacks the appropriate NICU level, or if a neonatologist fails to act on available data, that failure becomes its own basis for liability.
Transport Teams
Negligence can also occur during the ambulance or helicopter transfer itself. If monitoring equipment malfunctions, if a transport nurse fails to manage the baby’s airway, or if critical medications are not administered, the en-route care provider may share in the liability.
The potential parties in a transfer failure case may include:
- The attending obstetrician or midwife who failed to order the transfer
- The birth center that did not maintain a compliant transfer agreement
- The hospital that caused administrative delays in accepting the patient
- The transport team responsible for en-route care
- The receiving hospital’s NICU team for post-transfer errors
- Nursing staff who failed to escalate concerns through the chain of command
Under the Texas Civil Practice and Remedies Code Chapter 74, medical malpractice claims in Texas follow specific procedural requirements, including providing expert testimony and meeting expert report deadlines to keep a case alive. Working with a Texas High-Risk Pregnancy Transfer Failure Lawyer who understands these requirements from the outset is essential.
Texas Birth Center Transfer Requirements and Midwife Obligations
Texas law imposes specific obligations on licensed birth centers and midwives. Birth centers must maintain written transfer agreements with nearby hospitals to ensure safe, timely transfers during emergencies. Under Texas Administrative Code Rule 115.115, midwives are required to initiate immediate emergency transfer when certain high-risk conditions are identified during labor or delivery, including prolapsed cord, uncontrolled hemorrhage, and preeclampsia.
If a birth center operates without a valid transfer agreement, or if the facility is too far from a hospital to allow for safe transport during an emergency, the center may be in violation of state regulations. Violations of these midwife regulations can form a strong foundation for a medical negligence claim. Midwives practicing in birth center settings are expected to recognize when prenatal care alone is no longer sufficient and when the patient’s condition requires hospital-level intervention.
Damages Available in a Birth Injury Transfer Case
Damages in Texas birth injury cases may cover past and future medical expenses, life care planning, pain and suffering, and loss of earning capacity for the child, though non-economic damages are subject to state caps under Texas tort reform. Damages represent the financial and personal compensation sought in a legal claim.
Economic Damages (Uncapped)
Economic damages reflect the actual financial cost of the injury. In birth injury cases involving conditions like cerebral palsy or brain injury caused by oxygen deprivation, these costs can extend across the child’s entire lifetime. A Texas High-Risk Pregnancy Transfer Failure Lawyer at our firm places significant emphasis on thoroughly documenting:
- Past and future medical expenses, including surgeries, hospitalizations, and NICU costs
- Physical therapy, occupational therapy, and speech therapy
- Adaptive equipment such as wheelchairs, communication devices, and home modifications
- In-home nursing care and attendant care services
- Loss of future earning capacity if the child’s injuries prevent employment
- A professional life care plan that projects the total cost of care over the child’s expected lifespan
These damages are not subject to any cap in Texas, and they often represent the largest component of a birth injury recovery. Every dollar of future care must be supported by medical evidence and expert projections to ensure the child’s long-term needs are met.
Non-Economic Damages (Capped)
Non-economic damages compensate for physical pain, mental anguish, disfigurement, and physical impairment. Under Texas tort reform, these damages are capped at approximately $250,000 per individual provider and $500,000 per institution, with a combined maximum of roughly $750,000 in most cases.
Jaundice and Kernicterus
In some transfer cases, injuries are compounded by conditions like severe jaundice that goes untreated after birth. If jaundice progresses to kernicterus, a form of brain damage caused by excessive bilirubin levels, it can result in permanent neurological harm that adds substantially to the lifetime cost of care.
Tenfold NICU Medication Errors and Dosage Mistakes
One of the lesser-known risks in neonatal care involves medication dosing errors in the NICU. Because newborns require weight-based dosing calculated in fractions of adult amounts, a misplaced decimal point can result in a tenfold dosing error, meaning the baby receives ten times the intended dose. This massive overdose is a critical failure.
A study published in Frontiers in Pediatrics on pharmaceutical validation in NICUs found that prescribing errors are alarmingly common in neonatal settings, even under the supervision of a neonatologist. These errors can cause seizures, organ damage, or death, and they may compound the harm already caused by a delayed transfer. When a baby arrives at the NICU already compromised by oxygen deprivation, a medication error can turn a survivable injury into a catastrophic one. Our team reviews pharmacy records and medication administration logs as part of every NICU-related investigation.
How Our Texas Transfer Failure Lawyers Investigate Negligence
We utilize a team of in-house nurse consultants and board-certified patient advocates to audit transfer logs, electronic fetal monitoring strips, and communication records to identify the exact moment the standard of care was breached. Investigations in medical malpractice cases involve a thorough review of clinical records.
Reconstructing the Timeline
The first step in any transfer failure investigation is building a minute-by-minute timeline. Electronic fetal monitoring (EFM), the continuous recording of fetal heart rate and uterine activity during labor, produces a detailed paper or digital trail. We review those strips alongside nursing notes, physician orders, and hospital admission and discharge records to determine when distress was present, when it was recognized (or missed), and when action was finally taken.
Hospitals and transport teams often operate on slightly different clocks. We synchronize these records to create a unified master timeline. Discrepancies of even a few minutes can reveal attempts to cover up a delay.
Engaging the Right Experts
Our firm maintains a national network of medical experts, including maternal-fetal medicine specialists, neonatologists, and labor and delivery nurses, who provide objective case reviews and, when needed, expert testimony. These experts evaluate whether the care provided met accepted medical standards and whether the delay caused or contributed to the injury. Because medical malpractice cases are complex, we rely on specific insights.
To prove medical negligence, we must show exactly how the provider deviated from the standard of care. Our investigation typically includes:
- Review of all electronic fetal monitoring strips from labor and delivery
- Analysis of nursing notes and chain-of-command communications
- Audit of transfer request logs, transport team dispatch records, and arrival times
- Examination of the receiving hospital’s NICU records, including cooling therapy initiation times
- Review of pharmacy and medication administration records for dosing accuracy
- Consultation with qualified medical experts to establish causation
No Upfront Cost
We handle these cases on a contingency fee basis. That means you pay no attorney fees and no investigation costs unless we recover compensation on your behalf. The financial risk of pursuing answers should never be a barrier for a family that has already been through so much. As a Texas High-Risk Pregnancy Transfer Failure Lawyer, we assume the financial risk so you can focus on your family. Our Board Certified Patient Advocates support you through this process.
Texas Statute of Limitations for Birth Injury Transfer Claims
Generally, medical malpractice claims in Texas must be filed within two years of the negligence, but exceptions exist for minors allowing claims to be filed until the child reaches age 14 in certain circumstances. If you are considering speaking with a lawyer for high-risk pregnancy transfer failure in Texas, understanding the filing deadlines is one of the most time-sensitive steps you can take.
The Two-Year Rule
Statutes of limitations are legal deadlines that restrict the time you have to file a lawsuit. Under Texas law, the two-year window typically begins on the date of the birth event for parents pursuing their own claims, such as loss of consortium or emotional distress. While Texas tort reform/damage caps restrict the amount you can recover, the statute of limitations restricts the time you have to file a lawsuit at all. Missing this deadline generally bars recovery for parental claims forever.
The Minors Exception
Texas law provides an extended filing window for claims brought on behalf of an injured child. Understanding the minor statute of limitations can be confusing for parents. In certain circumstances, a birth injury claim can be filed on behalf of the minor until the child reaches age 14. This extension recognizes that many birth injuries, particularly those involving brain damage, may not be fully diagnosed until months or years after delivery.
The Statute of Repose
Even with the minors exception, Texas imposes an absolute outer limit known as the statute of repose. This deadline is set at 10 years from the date of the negligent act. Once 10 years have passed, the right to file is generally extinguished regardless of when the injury was discovered.
This is a strict deadline. Even if the injury was not discovered until age 11, the claim may be barred if the negligence occurred more than 10 years prior. Because these deadlines can overlap and exceptions can be fact-specific, have your case evaluated as early as possible to preserve your family’s legal options.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
If your child suffered a preventable injury connected to a delayed transfer or NICU error, you deserve a legal team that understands both the medicine and the law. Hastings Law Firm focuses exclusively on medical negligence, and our team of attorneys, nurse consultants, and patient advocates is prepared to review what happened and help your family understand the path forward.
We represent families across Texas from offices in Houston, The Woodlands, Dallas, and Austin, and we handle cases nationwide through our co-counsel network. Every confidential evaluation is free, and you pay nothing unless we recover compensation for your family.
Contact us today for a risk-free case evaluation. Let us help you find the answers you deserve.
Frequently Asked Questions About High-Risk Pregnancy Transfer Failure in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
