

Texas Group B Streptococcus Birth Injury Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
A preventable Group B Streptococcus infection in a newborn can leave families facing overwhelming fear, prolonged intensive care, and lasting harm when screening, antibiotics, or monitoring fall short. Medical teams have established protocols for prenatal testing and intrapartum antibiotics, and failures to follow them can turn a manageable risk into a severe infection. Understanding how missed screening, delayed treatment, and ignored warning signs happen can help families make sense of what went wrong. If you or a loved one were harmed or worse due to Group B Streptococcus birth injury in Texas, contact Hastings Law Firm for a free, confidential case review.

Advocating for Families Harmed by Preventable Infant Infections
What You Should Know About Infant GBS Infection Negligence Claims in Texas:
- Lasting harm can follow when a newborn Group B Streptococcus infection is not prevented or treated promptly.
- Preventable injury may be indicated when screening is missed, results are ignored, or antibiotics are delayed during labor.
- Severe outcomes can include brain damage, neurologic damage, and extended NICU stays.
- Accountability can extend beyond physicians because nurses have an independent duty to escalate safety concerns when protocols are not followed.
- Options can be lost if Texas requirements for medical malpractice claims are not met.
- Recovery can be shaped by limits and rules that apply to healthcare liability claims in Texas.
- Compensation may focus on long term needs when a child has permanent impairment requiring ongoing care.
- Disputes often turn on what the medical record shows about screening status, antibiotic choice, and response to warning signs.
- Key evidence may include nursing notes, communication logs, fetal monitoring strips, lab results, and NICU admission records.

A Healthcare Focused Law Firm
When a newborn develops a serious infection that proper screening and timely treatment could have prevented, the emotional toll on a family is immense. You may be facing a NICU stay, uncertain prognoses, and a growing sense that something was missed along the way. Those feelings deserve to be taken seriously.
Group B Streptococcus, commonly called GBS, is one of the leading causes of life-threatening infections in newborns. The medical community has well-established protocols for screening and prevention. When those protocols are not followed, the consequences can be devastating and permanent.
As a Texas Group B Streptococcus birth injury lawyer, Hastings Law Firm focuses exclusively on medical malpractice cases, including preventable neonatal infections caused by failures in GBS screening and treatment. If your child was harmed by what you believe was a preventable GBS infection, we can review what happened and explain your legal options in a free, confidential consultation.
How Medical Negligence Leads to Severe GBS Infections
Medical negligence in GBS cases typically occurs when a healthcare provider fails to screen the mother, fails to administer prophylactic antibiotics during labor, or fails to recognize infection symptoms in the newborn after delivery.
Group B Streptococcus (GBS) is a type of bacteria that can be carried in the gastrointestinal and genital tracts of healthy adults without causing symptoms. The danger arises during childbirth. Through vertical transmission, the passage of bacteria from mother to baby during labor and delivery, a newborn can be exposed to GBS as it moves through the birth canal. Without preventive treatment, this exposure can lead to severe neonatal infection.
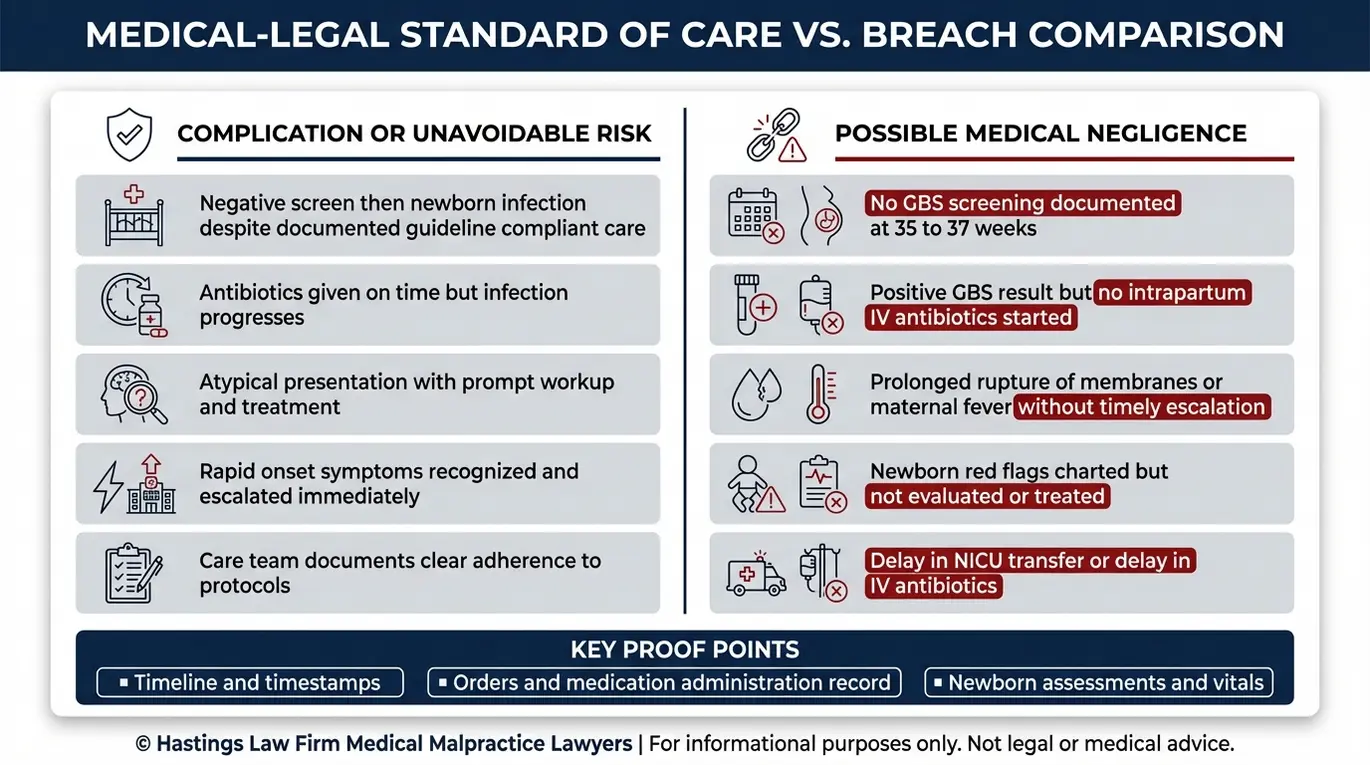
Not every GBS exposure results in illness, and not every neonatal infection is the result of malpractice. The distinction between an unavoidable complication and actionable medical malpractice depends on whether the medical team met the standard of care, the level of treatment a reasonably competent provider would deliver under similar circumstances.
When the standard of care is met and an infant still develops an infection, that may be an unavoidable complication. But when a provider skips universal screening, ignores a positive GBS result, or fails to start antibiotics during labor, the resulting infection may be preventable. A birth injury lawyer in Texas helps families understand their rights in these circumstances.
The outcomes of untreated GBS in newborns can be severe. According to the CDC’s Early Onset Neonatal Sepsis Surveillance data, GBS remains a significant cause of neonatal sepsis. Left unchecked, these infections can progress to brain damage, neurologic damage, and extended NICU (Neonatal Intensive Care Unit) stays that reshape a family’s life permanently.
| Unavoidable Complication | Actionable Medical Malpractice | |
|---|---|---|
| GBS Screening | Screening performed on time; results properly documented | Screening missed, delayed, or results lost/ignored |
| Antibiotic Administration | Antibiotics given per protocol; infection still occurs | Antibiotics not ordered, delayed, or wrong drug administered |
| Newborn Monitoring | Symptoms recognized and treated promptly | Warning signs dismissed or not escalated |
| Outcome | Harm despite proper care | Harm that proper care could have prevented |
Independent Nursing Duty to Advocate
Nurses are not simply order-followers. They carry an independent professional duty to advocate for patients, including newborns who cannot advocate for themselves. If a physician fails to order intrapartum antibiotic prophylaxis (IV antibiotics during labor) for a GBS-positive mother, a nurse who is aware of the positive status has a responsibility to question that omission and escalate the concern.
This independent duty is part of the nursing standard of care. Nurses must use the chain of command to report safety concerns to a charge nurse or supervisor if the attending doctor ignores established protocols. This advocacy is the last line of defense for a vulnerable newborn.
In our investigations, we examine nursing notes, communication logs, and chain-of-command documentation to determine whether bedside nurses raised the alarm or remained silent when a critical step was missed. A lawyer for Group B Strep negligence can analyze these logs to determine if this duty was upheld. Our in-house medical team includes former hospital nurses who provide insider insight into how these errors happen and how hospital protocols are often ignored.
The Standard of Care Regarding Screening and Antibiotics
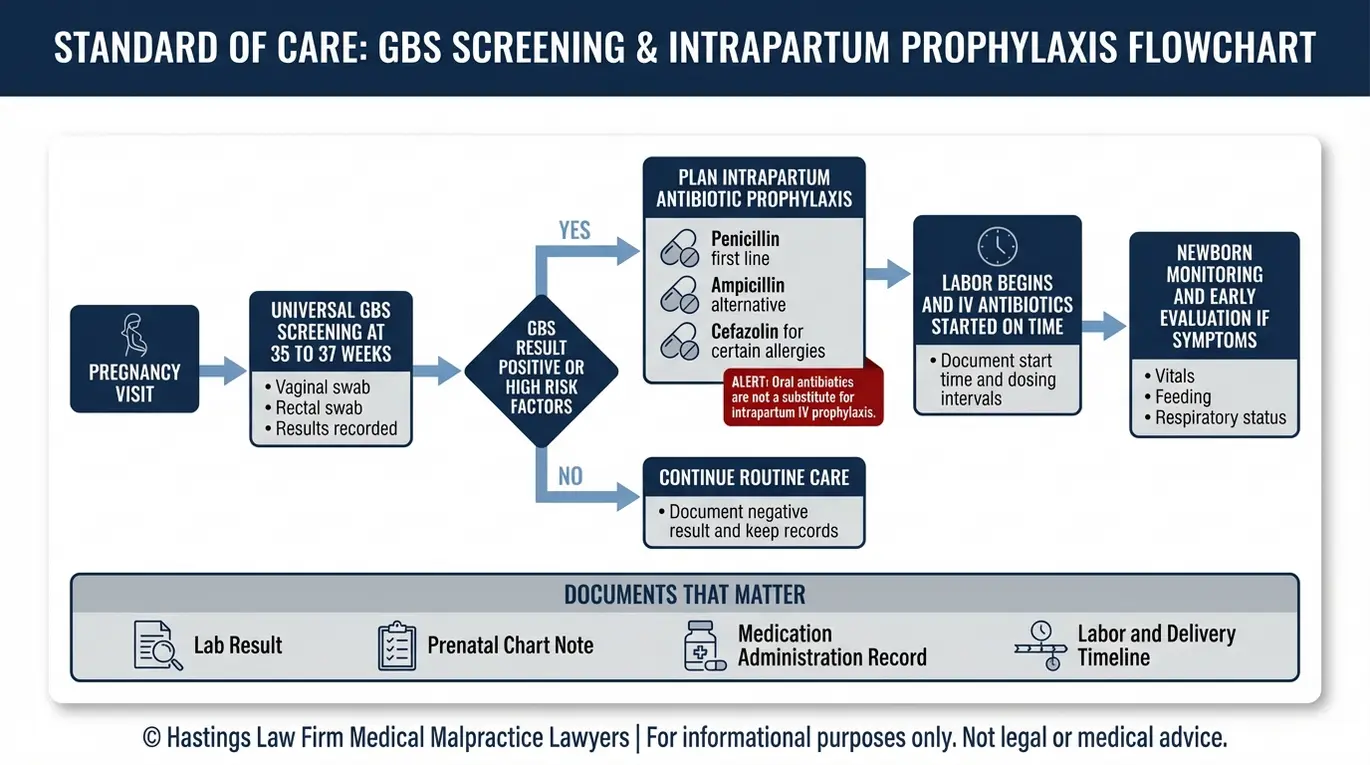
The standard of care mandates universal screening for GBS between 36 0/7 and 37 6/7 weeks of gestation and the administration of IV antibiotics during labor for mothers who test positive.
This screening is performed using a vaginal swab and rectal swab, a simple test where a provider collects samples from the lower vagina and rectum to detect GBS colonization. In some cases, GBS bacteriuria, the presence of GBS detected through a routine urine culture, identifies heavy colonization earlier in pregnancy. Either result should trigger a clear plan for antibiotic treatment during labor.
Research published in a study on perinatal GBS disease trends after updated screening recommendations confirms that universal prenatal testing and appropriate antibiotic use during labor have significantly reduced early-onset GBS infections. When providers follow the protocol, the risk drops substantially. When they do not, infants face preventable harm.
For GBS-positive mothers, the standard of care requires intrapartum antibiotic prophylaxis (IAP), the administration of IV antibiotics during active labor to reduce bacterial transmission. The preferred drug is penicillin. When a patient has a penicillin allergy, providers should select an appropriate alternative based on the severity and type of allergy. For patients with a history indicating low risk of anaphylaxis, cefazolin is recommended. For those with high risk of anaphylaxis, clindamycin is used if the GBS isolate is known to be susceptible; otherwise, vancomycin may be administered. A study on antibiotic selection for GBS prophylaxis among penicillin-allergic patients highlights the importance of proper allergy assessment and drug selection in both academic and community hospital settings.
A GBS birth injury attorney investigates whether each of these steps was completed correctly and on time. For families working with a lawyer for infant infection cases, the medical records often tell a clear story about what was done and what was missed.
Standard of Care Checklist for GBS Prevention:
- Universal GBS screening performed between 36 0/7 and 37 6/7 weeks of gestation
- Vaginal-rectal swab culture collected and properly processed
- Urine cultures reviewed for GBS bacteriuria throughout pregnancy
- Positive GBS status clearly documented in the medical record and communicated to the labor and delivery team
- IV antibiotics (penicillin for non-allergic patients; cefazolin for low-risk penicillin allergy; clindamycin or vancomycin for high-risk allergy based on susceptibility testing) initiated during labor, ideally at least four hours before delivery
- Continuous monitoring for maternal and neonatal signs of infection throughout labor and after birth
Oral vs. Intravenous Antibiotics: Efficacy
One critical distinction that can determine the outcome for a newborn is the route of antibiotic delivery. Oral antibiotics are generally insufficient for GBS prophylaxis (preventative treatment) during labor. This is because oral medications take significantly longer to reach effective concentrations in the bloodstream and cannot be relied upon to cross the placenta rapidly enough to protect the fetus during delivery.
The standard of care calls for IV antibiotics administered directly into the bloodstream during active labor. By contrast, IV administration achieves high therapeutic levels in the maternal bloodstream almost immediately, ensuring the baby is protected. If a provider prescribes oral antibiotics instead of IV antibiotics for a GBS-positive mother in labor, that deviation from protocol may constitute medical negligence. Texas birth injury legal counsel at Hastings Law Firm can evaluate whether the method of antibiotic delivery fell below the accepted standard.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Identifying Risk Factors and Missed Symptoms in Newborns
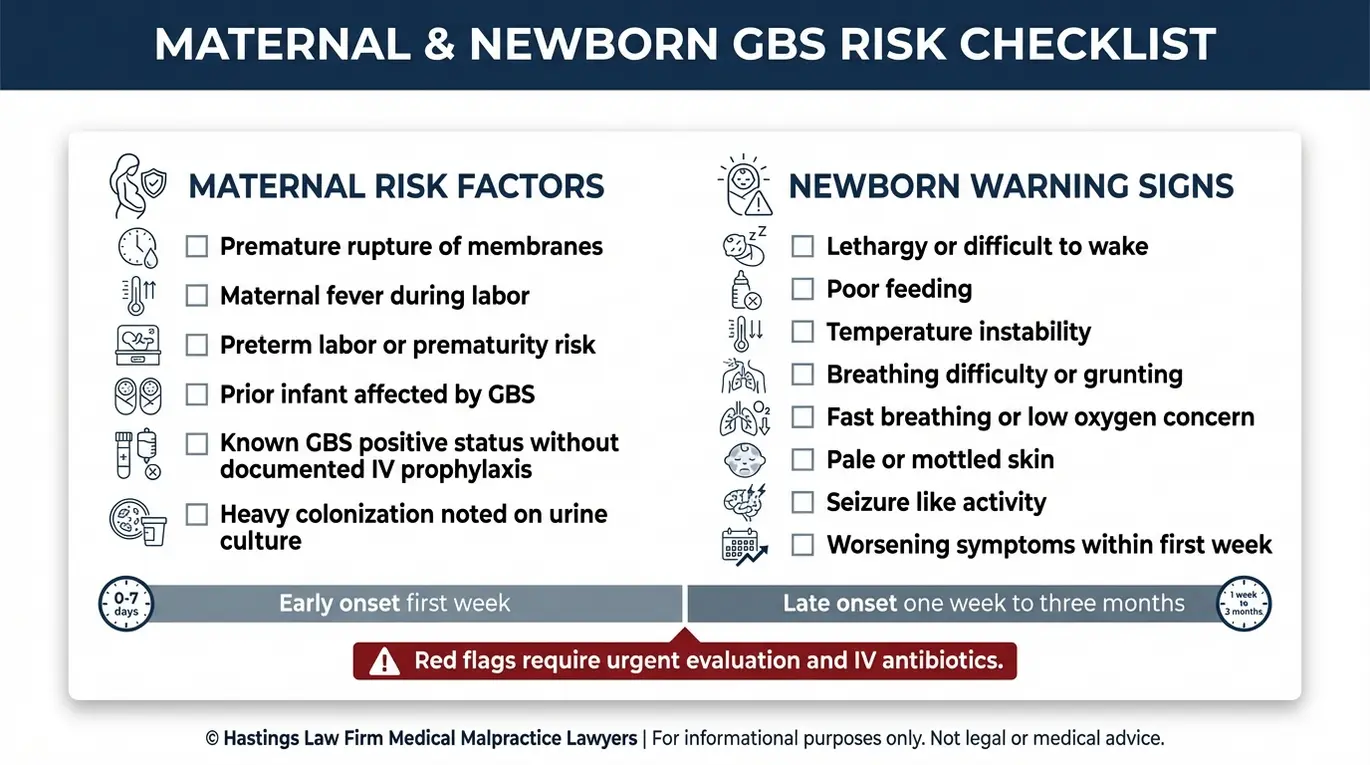
Doctors and nurses must monitor for risk factors such as maternal fever, premature rupture of membranes (PROM), and prematurity, as well as newborn symptoms like lethargy, breathing difficulties, and poor feeding.
GBS disease in newborns presents in two forms. Early-onset GBS disease develops within the first week of life, most commonly in the first 24 hours, and results from bacterial exposure during labor and delivery. Late-onset GBS disease appears between one week and three months of age and may be acquired from environmental or other sources.
For early-onset disease, certain maternal risk factors significantly raise the risk. These include premature rupture of membranes (PROM), the breaking of the amniotic sac before labor begins, maternal fever during labor, a prior infant with GBS disease, and preterm delivery before 37 weeks. PROM is particularly dangerous because once the amniotic sac ruptures, the sterile environment protecting the baby is gone, allowing bacteria to ascend and infect the fetus before birth. When any of these factors are present, the care team should be on heightened alert.
According to the CDC’s overview of Group B Strep symptoms, newborn Warning Signs can escalate quickly. If symptoms are dismissed or not acted upon in time, a treatable infection can progress to sepsis, pneumonia, or meningitis. Time is the enemy in these scenarios. A neonate’s condition can deteriorate from stable to critical in a matter of hours.
Providers must not only identify these signs but react with immediate urgency. Septic shock and lasting neurologic injury may follow. A Texas malpractice lawyer experienced in GBS cases examines whether the care team identified and responded to these warning signs appropriately.
An infant infection attorney at Hastings Law Firm reviews fetal monitoring strips, nursing assessments, lab results, and NICU admission records to build a detailed timeline of what the medical team knew and when they knew it.
| Warning Signs | |
|---|---|
| Mother (During Labor) | Fever (temperature ≥ 100.4°F), premature rupture of membranes, prolonged labor after membrane rupture (≥18 hours), preterm labor before 37 weeks, previous GBS-positive pregnancy |
| Newborn (After Delivery) | Grunting or labored breathing, lethargy or limpness, temperature instability (fever or hypothermia), poor feeding or refusal to eat, irritability, jaundice appearing within hours of birth |
Filing a Birth Injury Lawsuit Under Texas Law
Filing a lawsuit in Texas involves meeting strict deadlines, such as the statute of limitations, and fulfilling Chapter 74 requirements, including the submission of an expert report within 120 days of filing. Understanding these requirements early is essential to protecting your family’s claim.
Texas Chapter 74 governs all healthcare liability claims in the state. One of its most important requirements is the expert report, a written opinion from a qualified medical expert that must be served within 120 days of filing the lawsuit. This statute places a heavy burden on plaintiffs to prove their case early in the litigation process.
The expert report cannot be a vague assertion of fault. It must offer a granular analysis of the medical records and identify the applicable standard of care. The expert must then explain how the provider deviated from that standard and how the deviation caused the injury. If the report is not filed on time or does not meet the statutory requirements, the case can be dismissed.
The general statute of limitations for medical malpractice in Texas is two years from the date of the negligent act. Our founder, Tommy Hastings, is Board Certified in Personal Injury Trial Law by the Texas Board of Legal Specialization, a distinction held by fewer than 2% of attorneys in the state. Because birth injury deadlines are strict and fact-specific, consulting a Texas birth injury lawyer as early as possible helps ensure no filing windows are missed.
Recoverable damages in a GBS birth injury case may include past and future medical expenses, the cost of a life care plan for children with permanent disabilities, lost earning capacity, physical impairment, pain and suffering, and mental anguish. Life care plans are particularly critical in GBS cases resulting in cerebral palsy or severe brain damage. These plans project the costs of therapies, home modifications, and 24-hour attendant care that a child may require for the rest of their life. Our team works with medical experts and life care planners to document the full scope of your child’s needs.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
GBS infections in newborns are among the most preventable complications in modern obstetric care. When screening is missed or antibiotics are not administered, the consequences fall on the smallest and most vulnerable patients and the families who love them.
At Hastings Law Firm, our legal and medical team, including in-house nurse consultants and board-certified trial attorneys, investigates these cases from day one with the rigor needed to hold providers accountable. We advance all case costs, and you pay no attorney fees unless we recover compensation for your family.
If your child suffered a serious infection that you believe could have been prevented, reach out to our team for a free, confidential case evaluation. As a Texas Group B Strep lawyer, we can review your medical records, identify what went wrong, and help you understand the path forward. Contact Hastings Law Firm today.
Frequently Asked Questions About Group B Streptococcus Birth Injury in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
