

Texas Fetal Monitoring Malpractice Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: May 6, 2026
Fetal monitoring during labor is meant to warn a medical team when a baby is not tolerating labor well. When warning patterns on electronic fetal monitoring strips are missed, misread, or not acted on quickly, families can be left facing permanent injury, lifelong care needs, and overwhelming uncertainty about what happened in the delivery room. Understanding how fetal heart rate tracings are interpreted and how nurses and obstetricians are expected to respond can clarify where care may have broken down. If you or a loved one were harmed or worse due to fetal monitoring errors in Texas, contact Hastings Law Firm for a free, confidential case review.
Top Rated Birth Injury Attorneys Helping Families Across Texas
What You Should Know About Electronic Fetal Monitor Negligence Claims in Texas:
- Permanent brain injury can result when fetal distress is not addressed in time and oxygen deprivation continues during labor.
- Lifelong financial and emotional burdens can follow severe birth injuries due to ongoing medical care, therapy, adaptive equipment, and specialized education needs.
- Disputes over responsibility can arise when concerning fetal monitor patterns are not escalated promptly from nursing staff to the attending obstetrician.
- Options for recovery in Texas can be limited for non economic harms because state law caps certain damages in medical malpractice cases.
- A valid claim can be lost if required case filings are not handled correctly because Texas law imposes strict procedural requirements.
- Hospitals may contest liability by arguing electronic fetal monitoring produces false positives, which can shift the focus to whether the team responded appropriately to the information available.
- Serious fetal distress patterns can be central to evaluating what went wrong, including absent variability and recurrent late decelerations.
- The need for an emergency C section can become urgent when bedside resuscitation measures do not restore a reassuring fetal heart rate pattern.
- Questions about equipment reliability can matter when external monitoring produces an unclear signal and internal monitoring is not used when indicated.
- Medical records such as fetal monitor strips, nursing notes, and communication logs can be pivotal for reconstructing timing and clinical decision making.

A Healthcare Focused Law Firm
When a baby suffers a preventable injury during labor and delivery, families are often left with questions that no one at the hospital is willing to answer. You may sense that something went wrong with how the fetal monitor was read or how quickly the medical team responded, but proving it requires medical and legal knowledge that most people simply do not have.
Founded by board-certified trial attorney Tommy Hastings, our legal team focuses exclusively on medical malpractice. We include former defense attorneys who once represented hospitals and in-house nurse consultants who understand how labor and delivery units operate from the inside. We know what to look for in the records, and we know how to hold providers accountable.
If you believe your child was harmed by a failure to respond to fetal distress, contact Hastings Law Firm for a free, confidential case evaluation. We can review what happened and explain your options.
Establishing Negligence in Fetal Monitoring Errors
Medical malpractice occurs when healthcare providers fail to meet the standard of care, the level of treatment a reasonably competent professional would provide under similar circumstances, by ignoring, misinterpreting, or reacting too slowly to electronic fetal monitoring data that indicates a baby is in distress.
Fetal monitoring involves tracking the baby’s heart rate to identify potential risks during labor. Electronic fetal monitoring (EFM), the primary tool used during labor to track a baby’s heart rate alongside the timing and strength of uterine contractions, produces data known as fetal heart rate tracings or EFM strips. This data gives the medical team real-time information about how the baby is tolerating labor.
When those tracings show warning signs and the team fails to act, the result can be catastrophic. This concept is sometimes described as a “failure to rescue.” The monitor provided the information and the data showed the problem, but the medical team did not respond in time.
According to research published by PubMed Central on obstetrics and gynecology malpractice, obstetrical negligence claims frequently center on exactly this type of breakdown between available information and clinical action. Common errors fetal monitoring malpractice attorneys in Texas investigate include:
- Failing to recognize abnormal patterns on the EFM strip
- Misinterpreting the severity of decelerations or changes in heart rate
- Delaying notification to the attending obstetrician
- Ignoring monitor alarms or silencing them without clinical justification
- Failing to intervene or escalate care when the tracing deteriorates
Hospitals often challenge the reliability of EFM itself by arguing that the technology produces false positives. We anticipate this argument and counter it with expert testimony, clinical context, and a detailed review of what the strip actually showed in real time.
The question is not whether EFM is perfect; the question is whether the medical team responded appropriately to the information they had. A qualified Texas Fetal Monitoring Malpractice Lawyer knows how to address these defenses by proving that the specific patterns on the strip demanded action. This establishes the necessary elements of medical negligence, ensuring that valid claims are not dismissed due to technical arguments about equipment limitations. By focusing on the provider’s reaction to the data rather than the data’s potential for error, we demonstrate that the failure lay in human decision-making.
Recognizing Critical Signs of Fetal Distress on EFM Strips
Critical signs of fetal distress include absent baseline variability, repetitive late decelerations, and severe bradycardia, all of which can indicate the baby is suffering from oxygen deprivation.
These signs are visual indicators on a monitor strip that show whether a baby is receiving enough oxygen. Understanding these patterns starts with baseline variability, the normal, small fluctuations in a baby’s heart rate from beat to beat. Healthy variability signals that the baby’s nervous system is functioning well and receiving adequate oxygen.
When variability becomes minimal or disappears entirely, it may suggest the baby’s brain is no longer compensating for reduced oxygen, a condition known as hypoxia. Two types of decelerations are especially significant. Late decelerations, drops in heart rate that recover after the contraction ends, can indicate placental insufficiency.
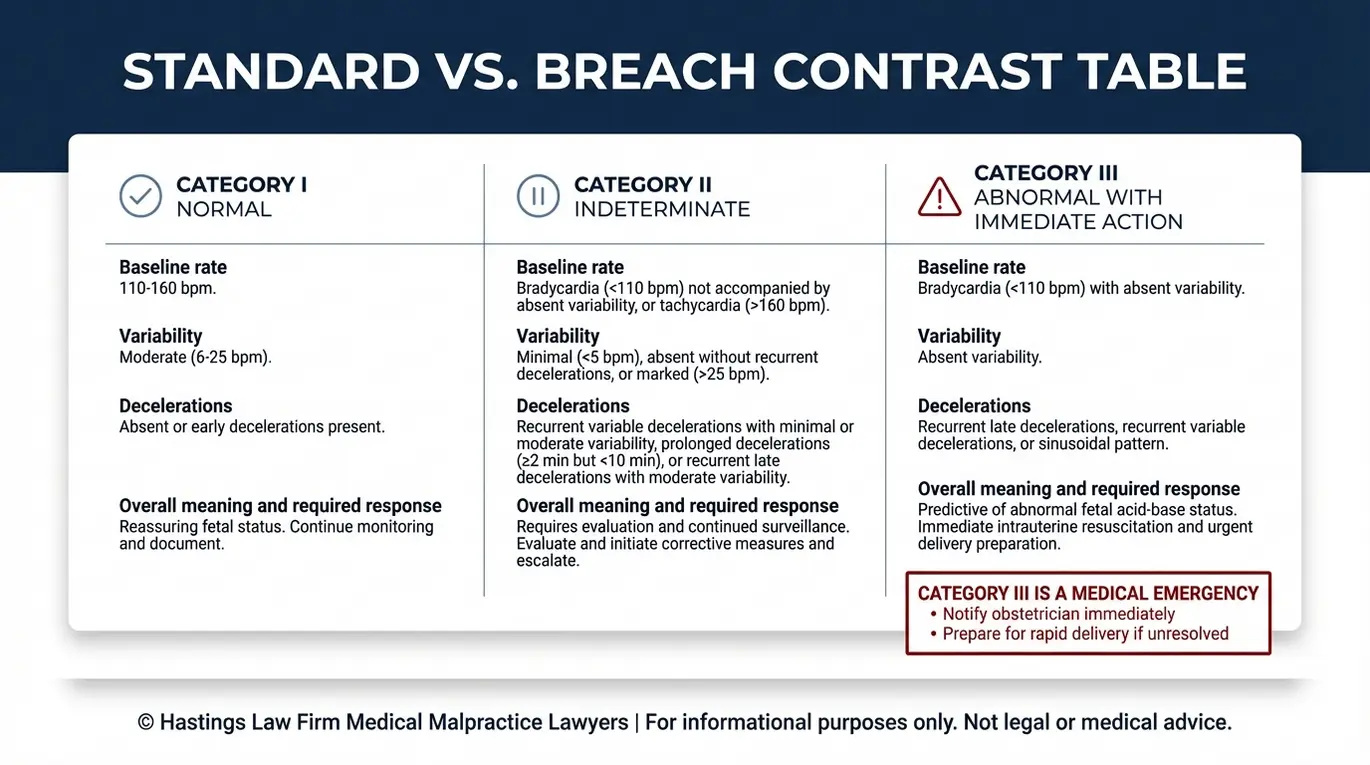
Variable decelerations are abrupt drops in heart rate often associated with umbilical cord compression. While occasional variable decelerations may be manageable, repetitive or worsening patterns demand close attention. Fetal heart rate tracings are classified into three categories based on guidelines outlined in the ACOG Clinical Practice Guideline published through Washington University:
| Category | Classification | Characteristics | Required Response |
|---|---|---|---|
| Category I | Normal | Normal baseline (110–160 bpm), moderate variability, no late or variable decelerations | Routine monitoring |
| Category II | Indeterminate | Minimal variability, recurrent variable decelerations, prolonged decelerations | Close surveillance, continued evaluation |
| Category III | Abnormal | Absent variability with recurrent late decelerations, bradycardia, or sinusoidal pattern | Immediate intervention required |
As detailed in a review of fetal heart rate classifications by the University of Alabama, Category III tracings are the most urgent. They indicate a high likelihood that the baby is experiencing oxygen deprivation. Clinical guidelines call for immediate action, including preparation for emergency delivery. Along with bradycardia, other abnormal heart rates like tachycardia (excessively fast heart rate) can also signal distress or infection requiring evaluation.
A common breakdown in care occurs when nurses monitoring the EFM strip do not escalate concerning patterns to the attending obstetrician quickly enough. A Texas fetal monitoring lawyer will examine the nursing notes, communication logs, and timing records to determine whether the chain of command functioned as it should have.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

The Standard of Care for Obstetricians and Nurses
The standard of care requires labor and delivery staff to perform continuous assessment, use intrauterine resuscitation techniques when distress is noted, and proceed to an emergency cesarean section (C-section) if the baby’s heart rate does not recover.
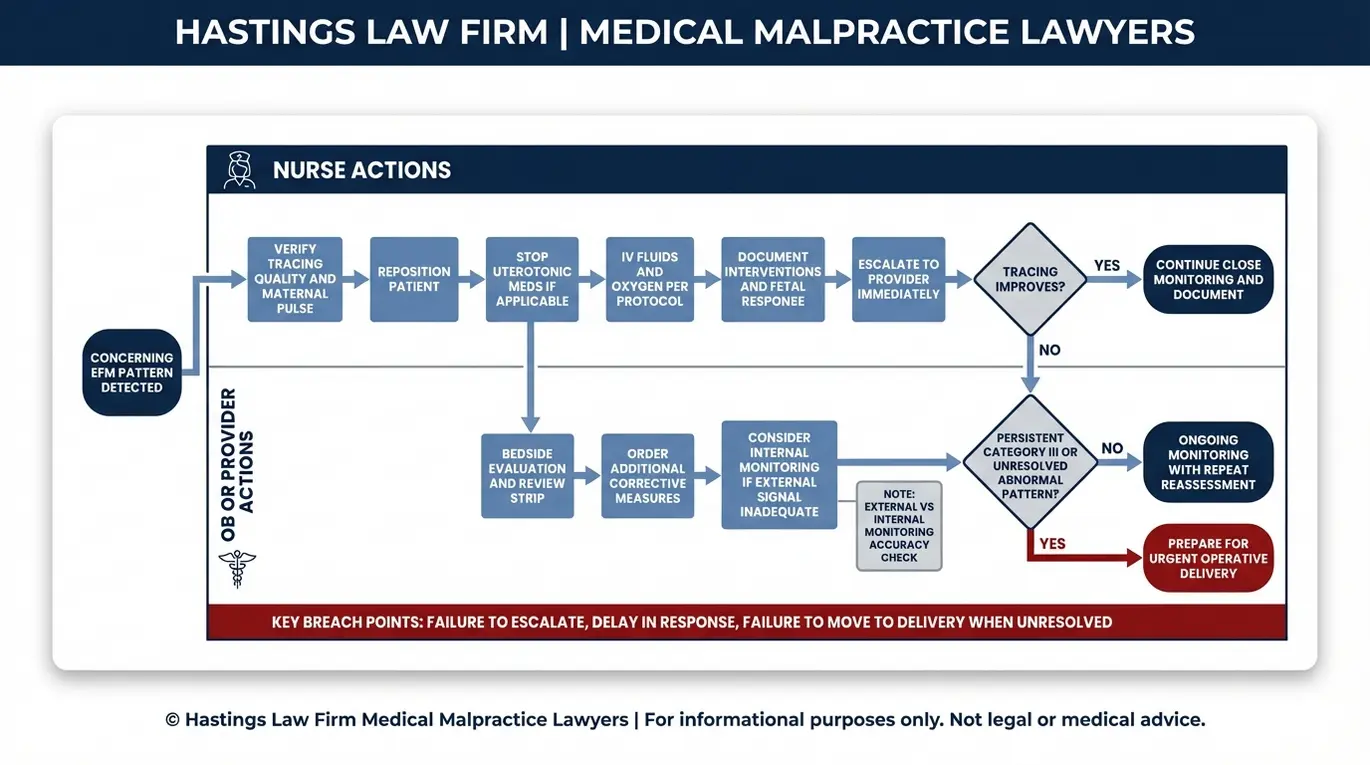
The chain of responsibility in a delivery room is clear. Nurses are responsible for continuous monitoring of the EFM strip and must promptly notify the attending obstetrician when they identify concerning patterns. The obstetrician must respond, assess the situation, and make timely decisions about intervention. A failure at any point in this chain can result in preventable harm.
When fetal distress is identified, the first response is typically intrauterine resuscitation. This refers to a set of bedside interventions designed to improve oxygen delivery to the baby before surgery becomes necessary. These steps include:
- Repositioning the mother (usually to her left side) to improve blood flow
- Administering supplemental oxygen to reverse oxygen deprivation
- Increasing IV fluids to support blood pressure and placental perfusion
- Discontinuing Pitocin or other labor-stimulating medications
- Performing an amnioinfusion if cord compression is suspected
If these measures do not restore a reassuring fetal heart rate pattern, the standard of care generally requires moving to an emergency C-section without unnecessary delay. We also consider the accuracy of the monitoring equipment itself. External fetal monitoring uses sensors placed on the mother’s abdomen, but it may sometimes provide an unreliable signal due to maternal obesity or fetal position changes.
When the external tracing is difficult to interpret, the standard of care may call for switching to internal fetal monitoring. This uses a fetal scalp electrode, a small sensor attached directly to the baby’s scalp that provides a more precise heart rate reading. We examine whether the clinical team made this switch when the situation called for it.
As outlined in Texas Civil Practice and Remedies Code, Chapter 74, establishing that a provider breached this standard requires qualified expert analysis. Malpractice lawyers for fetal monitoring errors work with board-certified obstetricians who can review the records and identify exactly where the standard of care was not met.
Permanent Injuries Caused by Delayed Emergency C-Sections
When fetal distress goes unaddressed for too long, the resulting lack of oxygen can cause permanent brain damage, leading to conditions such as hypoxic-ischemic encephalopathy (HIE) and cerebral palsy.
The mechanism of injury follows a specific progression. Oxygen deprivation, known medically as intrapartum hypoxia, reduces or cuts off the baby’s oxygen supply during labor. When hypoxia persists, it leads to ischemia, a dangerous reduction in blood flow to the brain.
Together, these conditions cause hypoxic-ischemic encephalopathy (HIE), the death or damage of brain tissue resulting from insufficient oxygen and blood flow. The severity of HIE depends largely on how long the deprivation lasted and how quickly the baby was delivered.
One of the most well-known outcomes of severe HIE is cerebral palsy, a group of permanent movement and posture disorders caused by damage to the developing brain. According to the Centers for Disease Control and Prevention (CDC), cerebral palsy is one of the most common motor disabilities in childhood.
For families, the diagnosis often means a lifetime of medical care, therapy, adaptive equipment, and specialized education. Lifetime care costs for a child with cerebral palsy can reach into the millions, covering physical therapy, occupational therapy, speech therapy, surgeries, medications, mobility devices, and home modifications.
Many families also need full-time caregiving support. Beyond the financial burden, non-economic damages account for the child’s pain and suffering, loss of enjoyment of life, and the profound emotional toll on the family.
Our attorneys evaluate the full scope of these losses, including any permanent brain injury, to ensure a family’s claim reflects both the immediate and long-term consequences of the injury. In the most tragic cases, these failures can lead to wrongful death.
Texas Laws Governing Electronic Fetal Monitoring Lawsuits
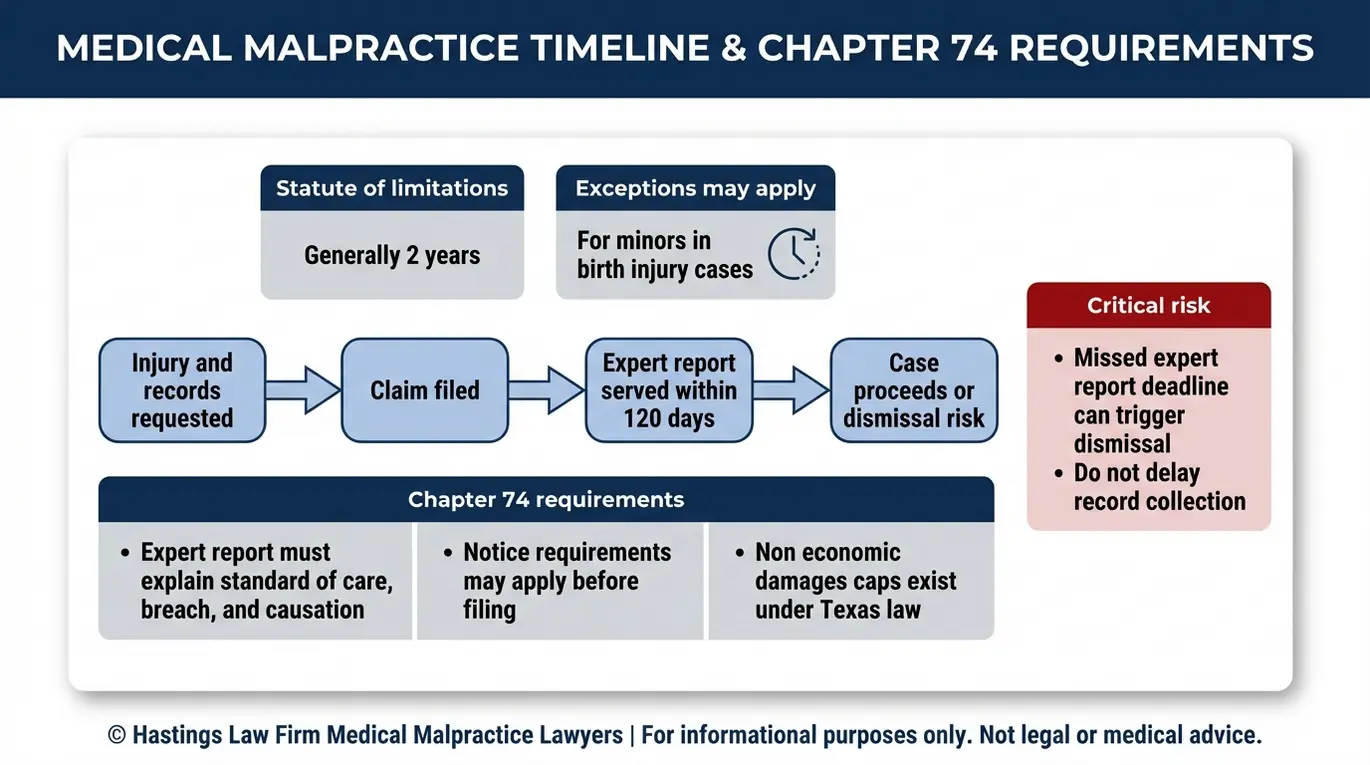
Texas law requires plaintiffs to serve an expert report within 120 days of filing suit and generally imposes a two-year statute of limitations, though exceptions exist for minors involved in birth injury cases.
These requirements are governed by Chapter 74 of the Texas Civil Practice and Remedies Code, also known as the Texas Medical Liability Act. The law was designed to screen out unsupported medical negligence claims, but it also creates procedural requirements that can end a valid case if they are not followed precisely. Working with a fetal monitoring malpractice law firm in Texas that handles these cases routinely helps manage these deadlines.
The expert report requirement is a significant hurdle. Within 120 days of filing, the patient must provide a written report from a qualified medical expert. This report details what the standard of care required, how it was breached, and how that breach caused the injury.
If this report is not served on time, the court can dismiss the case with prejudice, meaning it cannot be refiled. We work with a national network of board-certified obstetricians and maternal-fetal medicine specialists to prepare these reports.
Texas law also requires patients to provide pre-suit notice to each healthcare provider being sued at least 60 days before filing. This Notice of Claim triggers an opportunity for early resolution, but it also starts important timelines that must be managed carefully.
Families should also be aware of the damage caps Texas imposes on medical malpractice recoveries. Non-economic damages, which cover pain and suffering, are capped at $250,000 per physician and $250,000 per healthcare institution, with a combined cap of $500,000 for institutional defendants. Economic damages, such as medical costs and lost earning capacity, are not capped. While punitive damages are rare and typically reserved for cases involving gross negligence or malice, they may also be available in specific circumstances.
Texas Chapter 74: Key Requirements at a Glance
- Statute of Limitations: Two years from the date of injury (tolled for minors; subject to a 10-year statute of repose)
- Pre-Suit Notice: Must be sent to each defendant at least 60 days before filing
- Expert Report Deadline: Must be served within 120 days of filing suit
- Non-Economic Damage Caps: $250,000 per physician; $250,000 per hospital (up to $500,000 combined for institutions)
- Economic Damages: No cap
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
A birth injury caused by a failure to respond to fetal monitor warnings is not simply a complication. It is often a preventable event, and families deserve to know the truth about what happened in that delivery room.
At Hastings Law Firm, we treat every family with the empathy and transparency this moment demands. Our team of attorneys, nurse consultants, and medical experts will review your records, identify what went wrong, and build your case from day one as if it is going to trial.
We handle these cases on a contingency fee basis, which means you pay no attorney fees or costs unless we recover compensation for your family. If you are looking for a Texas fetal monitoring malpractice lawyer who will listen, investigate, and hold the responsible parties accountable, we are ready to help.
Call us today or request a free, confidential case evaluation online.
Frequently Asked Questions About Fetal Monitoring Errors in Texas

Key Fetal Monitoring Error Terms:
- Electronic fetal monitoring (EFM)
- A medical technology used during labor and delivery to continuously track the baby’s heart rate and the mother’s uterine contractions. EFM helps healthcare providers identify signs of fetal distress so they can intervene quickly if the baby is not getting enough oxygen. In malpractice cases, EFM data can show whether the medical team recognized warning signs and responded appropriately.
- Fetal heart rate tracings (EFM strips)
- The printed or digital records produced by electronic fetal monitoring equipment that display the baby’s heart rate patterns and the mother’s contractions over time. These strips serve as critical evidence in birth injury cases because they document whether healthcare providers saw warning signs of fetal distress and how quickly they acted.
- Baseline variability
- The normal fluctuations in a baby’s heart rate from beat to beat during labor, which indicate a healthy, well-oxygenated nervous system. When baseline variability decreases or disappears on fetal heart rate tracings, it can signal that the baby is not receiving adequate oxygen. Loss of variability is a serious warning sign that requires immediate medical attention.
- Late decelerations
- A pattern on fetal heart rate tracings where the baby’s heart rate drops after a contraction has already peaked, indicating that the placenta may not be delivering enough oxygen to the baby. Late decelerations are concerning because they suggest placental insufficiency, and when they occur repeatedly, they require urgent intervention such as repositioning the mother, administering oxygen, or performing an emergency cesarean section.
- Intrauterine resuscitation
- A set of emergency measures taken during labor to improve oxygen delivery to a distressed baby while the baby is still in the womb. These measures typically include repositioning the mother to relieve pressure on the umbilical cord, giving the mother supplemental oxygen, administering intravenous fluids, and stopping medications like Pitocin that strengthen contractions. Intrauterine resuscitation is the standard of care when fetal monitoring shows signs of distress.
- Fetal scalp electrode (internal fetal monitoring)
- A small monitoring device attached directly to the baby’s scalp through the cervix during labor to obtain more accurate readings of the baby’s heart rate than external monitoring. Internal fetal monitoring is used when external monitors provide unclear or unreliable tracings, or when the medical team needs precise information about the baby’s condition. The decision to switch from external to internal monitoring can be critical in malpractice cases involving fetal distress.
- Oxygen deprivation (intrapartum hypoxia)
- A condition during labor and delivery where the baby does not receive adequate oxygen, typically due to problems with the umbilical cord, placenta, or uterine contractions. When oxygen deprivation occurs during the birthing process and is not promptly addressed, it can lead to permanent brain damage. In malpractice cases, oxygen deprivation often results from delayed response to warning signs visible on fetal monitoring equipment.
- Hypoxic-ischemic encephalopathy (HIE)
- A type of permanent brain injury caused by insufficient oxygen and blood flow to the baby’s brain during labor and delivery. HIE can result in cerebral palsy, developmental delays, seizures, and other lifelong disabilities. This condition is often preventable when medical teams properly monitor fetal heart rate tracings and perform timely emergency cesarean sections in response to signs of fetal distress.
- Navigating the Complex Terrain of Obstetrics and Gynecology Malpractice Stakeholders, Expectations, and Legal Implications | PubMed Central
- Intrapartum Fetal Heart Rate Monitoring | obgyn.wustl.edu
- Review of Category I II and III Fetal Heart Rate Classifications | University of Alabama
- Civil Practice and Remedies Code Chapter 74 | Texas Legislature Online
- Data and Statistics for Cerebral Palsy | CDC
Get Answers Today
If you think that medical negligence, a dangerous drug, or a failed medical product caused harm to you or someone you love, our team is standing by to offer guidance. We’ll explain your options under current laws and help you move forward with clarity and understanding. Case reviews are free and 100% confidential.
