

Texas Cephalopelvic Disproportion Injury Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Obstructed labor linked to cephalopelvic disproportion can place a baby and mother at serious risk when warning signs are missed or delivery decisions are delayed. The condition may be hard to confirm early, but stalled labor and other documented findings can signal that the delivery plan needs to change. Mismanagement can lead to oxygen deprivation, traumatic injury, and lasting disability, and disputes often focus on whether the standard of care was met during prenatal assessment and active labor. If you or a loved one were harmed or worse due to cephalopelvic disproportion negligence in Texas, contact Hastings Law Firm for a free, confidential case review.
Experienced Advocacy for Victims of Obstructed Labor Negligence
What You Should Know About Obstructed Labor Negligence Claims in Texas:
- Lifelong neurological disability can result when obstructed labor is not addressed promptly and oxygen supply is reduced.
- Permanent physical injury can occur when excessive traction or instrument force is used during a delivery complicated by obstruction.
- Options for recovery in Texas can be limited for pain and suffering because non economic damages are capped.
- Financial recovery for long term care can be substantial because economic damages for medical costs and future care are not capped under Texas law.
- Disputes often turn on whether the care team responded appropriately once labor stopped progressing during active labor.
- Liability risk can increase when prenatal warning signs of a large baby or pelvic mismatch are not evaluated with appropriate testing.
- Severe harm can be associated with continuing vaginal delivery attempts when a timely C section is indicated.
- The risk of intracranial bleeding can rise when vacuum extraction is followed by forceps after the first method fails.
- Key records can be central to understanding what happened, including partogram entries and electronic fetal monitoring strips.

A Healthcare Focused Law Firm
When labor does not progress as it should, and a baby cannot safely pass through the birth canal, the decisions made by the medical team in those moments matter deeply. Obstructed labor, a condition where the baby’s passage through the pelvis is physically blocked, demands prompt recognition and decisive action. When that response is delayed or mismanaged, the consequences can change a family’s life forever. We understand the weight of these moments and are here to help you find the truth.
If your child was injured during a delivery involving obstructed labor, you may have questions about what went wrong and whether it could have been prevented. Founded in 2005 by Tommy Hastings, who is among the less than 2% of Texas attorneys board-certified in Personal Injury Trial Law, our firm focuses exclusively on medical malpractice. Our team includes in-house medical staff who can review what happened during your delivery. Contact us for a free, confidential case evaluation to understand your options.
Medical Negligence Involving Cephalopelvic Disproportion
Cephalopelvic disproportion (CPD) occurs when a baby’s head or body is too large to pass safely through the mother’s pelvis, leading to obstructed labor. Medical negligence arises when doctors fail to diagnose this mismatch or delay a necessary C-section, causing preventable birth injuries.
CPD itself is not malpractice; it is a medical condition. However, how a doctor responds can cross into negligence. A condition becomes a legal issue when a healthcare provider fails to meet the accepted standard of care, which is the level of treatment a reasonably competent professional would provide in the same situation.
One of the clearest warning signs of CPD is failure to progress, also known as labor dystocia, which refers to labor that stalls or slows significantly despite adequate contractions. When labor stalls, the medical team must evaluate why and adjust the plan. We investigate whether the provider recognized these signs and acted appropriately. A qualified lawyer for CPD birth injuries knows how to interpret these medical records to uncover critical details.
Medical negligence in CPD cases can take several forms:
- Failing to identify CPD risk factors during prenatal care
- Ignoring signs of labor dystocia during active labor
- Continuing vaginal delivery attempts when a Cesarean section is indicated
- Using excessive force or instruments on a baby that cannot safely deliver vaginally
According to Baylor University Medical Center Proceedings, a health care liability claim in Texas requires proof that a provider deviated from the accepted standard of care and that the deviation directly caused harm. In CPD cases, this often means showing that the medical team had enough clinical information to recognize the obstruction but did not change course.
Timing Challenges in Proving Negligence
Defense attorneys often argue that CPD is difficult to diagnose before or even during early labor. There is some truth to this. The fit between baby and pelvis is not always obvious until active labor begins. But that argument has limits.
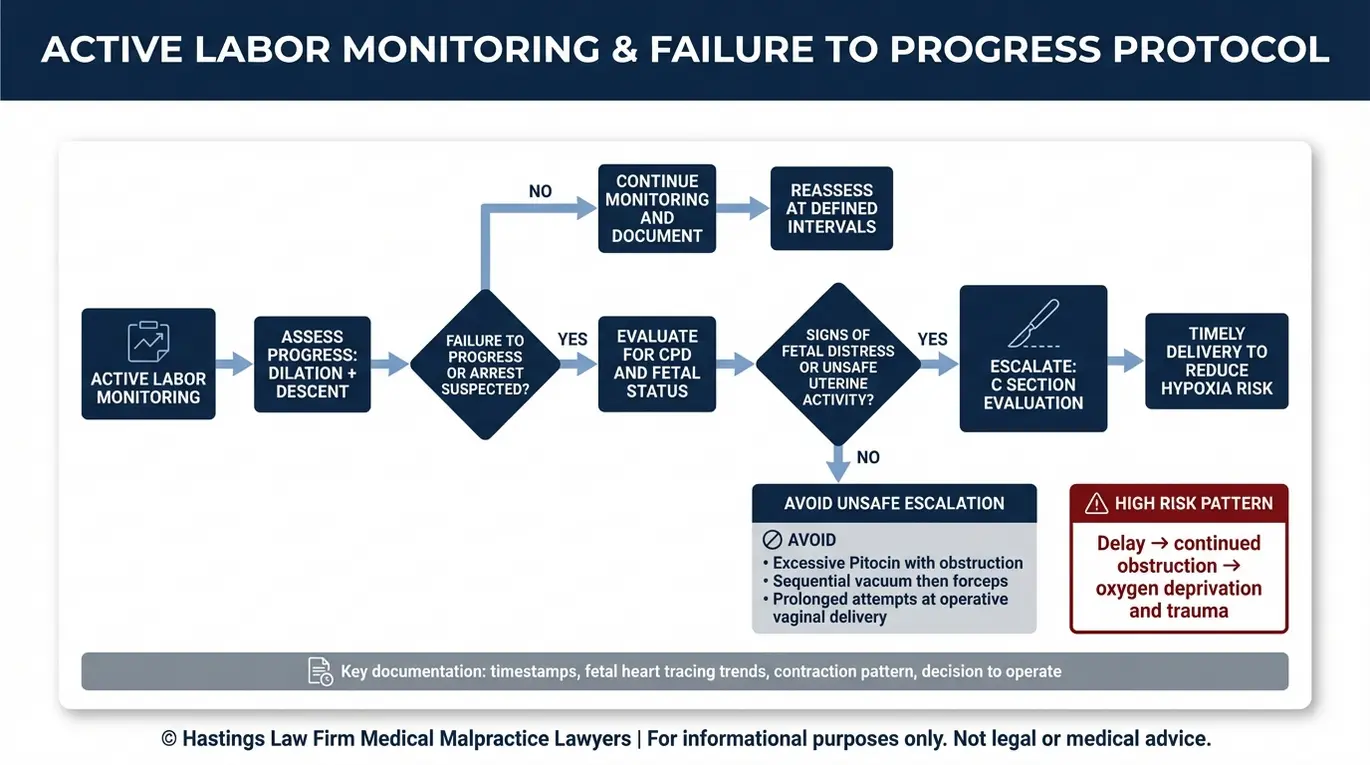
During active labor, providers should be tracking progress with tools like a partogram, which is a graphical record used to monitor cervical dilation and fetal descent over time. When the partogram shows that labor has stalled, that data creates a documented record of the problem. We examine whether the care team responded to those findings or continued down a path that was no longer safe. A pattern of inaction despite objective evidence of labor dystocia, or failure to progress, can be strong evidence of a breach in the standard of care.
Identifying Missed Risk Factors and Diagnosis Errors
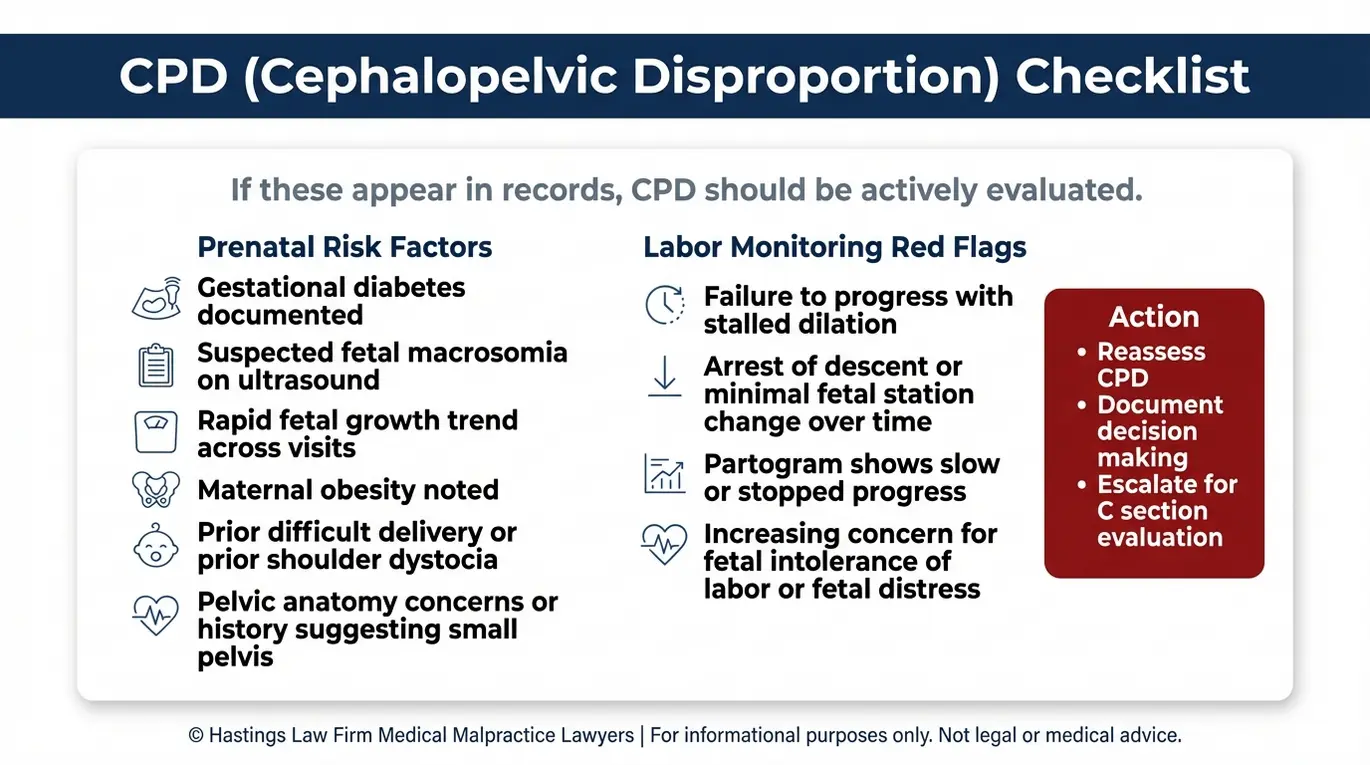
Doctors have a duty to assess risk factors such as fetal macrosomia, gestational diabetes, and maternal pelvic anatomy to anticipate potential obstruction. Failing to perform ultrasounds or ignoring warning signs during prenatal care can lead to liability if a birth injury occurs.
Several of these risk factors are identifiable well before delivery. Fetal macrosomia, a condition where the baby weighs more than 8 pounds 13 ounces, is one of the most significant. Research published in the Journal of Clinical Medicine confirms that ultrasound can help predict macrosomia in pregnancies complicated by diabetes mellitus, giving providers an opportunity to plan accordingly.
Pelvimetry, the clinical or imaging-based assessment of the mother’s pelvic dimensions, is another tool available to evaluate whether vaginal delivery is likely to succeed. While it is not always definitive on its own, it becomes especially relevant when combined with other risk factors.
During prenatal visits, doctors must also closely track the mother’s weight gain and fundal height. Differences in these measurements often signal that the fetus is larger than expected. If a provider dismisses these findings without ordering a growth ultrasound, they may miss a critical opportunity to diagnose macrosomia before labor begins. This failure to gather necessary data prevents the medical team from making informed decisions about the safety of a vaginal birth.
As a Texas Cephalopelvic Disproportion injury lawyer, we review whether the provider identified and acted on these warning signs. The following checklist outlines key risk factors that should prompt closer evaluation:
| Risk Factor | What the Provider Should Evaluate |
|---|---|
| Fetal macrosomia (estimated weight > 4,000g) | Ultrasound measurements; growth trends over multiple visits |
| Gestational diabetes | Blood sugar management; correlation with fetal size |
| Maternal obesity | Increased likelihood of large-for-gestational-age infant |
| Short maternal stature or small pelvic dimensions | Pelvimetry; clinical assessment of pelvic shape |
| History of difficult or obstructed deliveries | Review of prior birth records and outcomes |
| Post-term pregnancy (beyond 40 weeks) | Fetal growth monitoring; delivery planning |
| Failure to progress during labor | Partogram tracking; cervical dilation and fetal station |
When one or more of these factors is present and the provider does not adjust the delivery plan, the question shifts from whether this was a difficult delivery to whether it should have been managed differently. Our in-house medical staff reviews prenatal records, ultrasound reports, and labor documentation to determine whether the standard of care was met at every stage.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Standard of Care Violations During Delivery
The standard of care for unresolved CPD often requires a timely Cesarean section to prevent fetal distress. Negligence frequently involves the misuse of Pitocin to force labor or the dangerous application of forceps and vacuum extractors when a C-section is the safer option.
When labor stalls due to an obstruction, the safest course of action is often a C-section. A delay in making that call, sometimes referred to as arrest of descent, can expose both the mother and baby to serious harm. We examine exactly when the decision to proceed with surgery should have been made and whether the provider’s timeline fell below the accepted standard.
One of the most concerning patterns in these cases involves Pitocin, a synthetic form of oxytocin used to strengthen contractions. When used appropriately, Pitocin can help labor progress. But when the baby physically cannot fit through the pelvis, increasing contraction strength forces the uterus to push against an immovable obstruction. This can lead to uterine hyperstimulation, a condition where contractions become too frequent or too intense, potentially causing uterine rupture.
Instrument-assisted delivery raises similar concerns. Forceps and vacuum extractors can be appropriate tools in certain clinical situations. But when CPD is present and the baby cannot descend, applying mechanical force to the infant’s head carries significant risk of skull fractures, brain bleeds, and nerve damage. According to diagnostic criteria published by Clinical and Experimental Obstetrics & Gynecology, confirmed CPD should prompt surgical delivery rather than continued attempts at vaginal birth.
We look for the following red flags in medical records:
- Pitocin administered or increased after documented failure to progress
- Fetal heart rate decelerations that were not promptly addressed
- Vacuum extraction or forceps attempted despite signs of obstruction
- No documented reassessment of delivery plan after prolonged labor
- Absent or incomplete partogram entries during active labor
Dangers of Sequential Instrument Use
A particularly dangerous practice is sequential instrument use, where a provider attempts vacuum extraction and then switches to forceps when the first method fails. This approach dramatically increases the risk of intracranial hemorrhage, which is bleeding that occurs inside the skull. When CPD is present, the failure of one instrument should signal that vaginal delivery is not safe. Our team reviews delivery records closely to determine whether this pattern occurred.
Severe Birth Injuries Caused by Mismanaged CPD
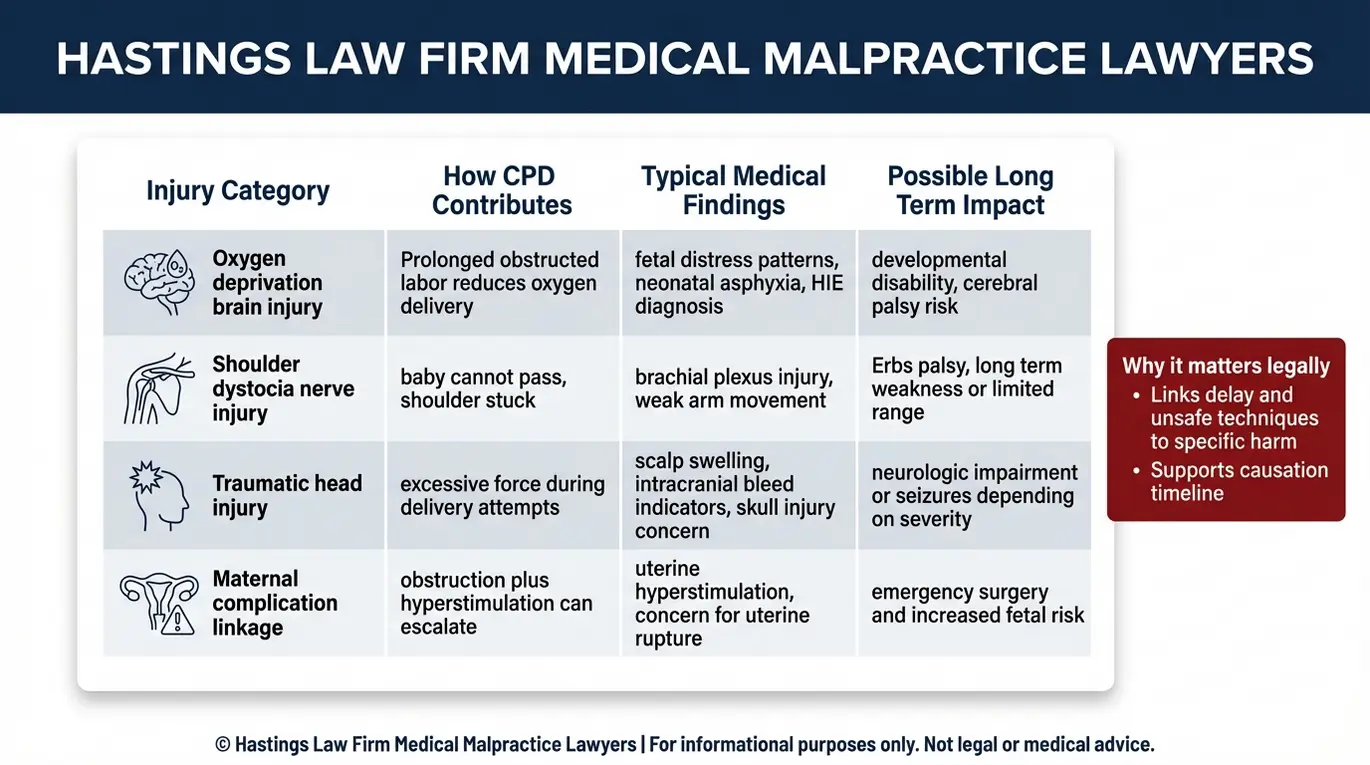
When CPD is not managed correctly, infants may suffer catastrophic injuries including Hypoxic-Ischemic Encephalopathy (HIE) from oxygen deprivation, traumatic brain injuries, or nerve damage such as Erb’s palsy from shoulder dystocia.
Prolonged obstructed labor can cause fetal distress, compress the umbilical cord, or disrupt placental blood flow, reducing the oxygen supply to the baby’s brain. If this oxygen deprivation continues long enough, it can lead to Hypoxic-Ischemic Encephalopathy, a type of brain injury caused by a combination of low oxygen and restricted blood flow. According to research published in Pediatrics, perinatal HIE remains a significant cause of long-term neurological disability. Children who survive moderate to severe HIE may develop cerebral palsy, seizure disorders, or other permanent conditions.
Physical trauma during delivery is another serious concern. When a baby’s shoulder becomes lodged behind the mother’s pubic bone, a complication known as shoulder dystocia, the maneuvers used to free the baby can injure the brachial plexus. This network of nerves runs from the neck through the shoulder and arm. Injury here can result in Erb’s palsy, which causes weakness or paralysis in the affected arm.
Excessive force during delivery, whether by hand or instrument, can also cause skull fractures and intracranial hemorrhages that lead to lasting developmental problems. We help families understand the connection between delivery decisions and the injuries their child sustained.
| Injury Type | How It Occurs | Potential Long-Term Impact |
|---|---|---|
| Hypoxic-Ischemic Encephalopathy (HIE) | Oxygen deprivation from prolonged labor or cord compression | Cerebral palsy, seizures, cognitive disabilities |
| Brachial Plexus Injury (Erb’s/Klumpke’s Palsy) | Nerve damage from shoulder dystocia or excessive traction | Arm weakness, limited mobility, possible paralysis |
| Skull Fractures / Intracranial Hemorrhage | Forceps or vacuum pressure on the skull | Developmental delays, neurological deficits |
| Neonatal Asphyxia | Severe oxygen deprivation at birth | Organ damage, long-term neurological impairment |
Securing Compensation for Birth Trauma in Texas Courts
Texas law allows families to recover economic damages for medical bills and future care, as well as non-economic damages for pain and suffering, though caps apply to the latter. A successful claim requires proving that the provider’s failure to manage CPD directly caused the child’s injury.
Recoverable economic damages for losses are not capped under Texas law and often represent the largest portion of recovery. These can include lifetime medical costs, therapy, assistive devices, and lost earning capacity. Our malpractice litigation team works with life care planning experts to calculate the true cost of the care a child will need over a lifetime.
Non-economic damages, which cover pain, suffering, and physical impairment, are subject to caps under Texas Civil Practice and Remedies Code Chapter 74. These limits are typically $250,000 per physician and $250,000 per hospital. While these caps can be frustrating, the uncapped economic damages in severe birth injury cases often far exceed those limits.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
Texas imposes strict deadlines on medical malpractice claims, and gathering the medical evidence needed to build a strong case takes time. If your child was injured during a delivery involving CPD, the sooner your records are reviewed, the better positioned your case will be.
Hastings Law Firm was founded on a simple belief: families deserve the truth about what happened and the accountability needed to prevent it from happening again. Our team includes in-house nurses, former defense attorneys, and board-certified trial lawyers who understand both the medicine and the law.
If you are looking for a Texas Cephalopelvic Disproportion injury lawyer, we are here to listen. Every consultation is free and confidential, and you pay no fees unless we recover compensation on your behalf. Contact us today to take the first step toward answers.
Frequently Asked Questions About Cephalopelvic Disproportion Injury in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
