

Texas Amniotic Fluid Embolism Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Amniotic fluid embolism is a rare obstetric emergency that can unfold without warning and quickly lead to catastrophic harm during labor or shortly after delivery. The most serious outcomes often turn on whether the medical team recognized early deterioration, escalated care immediately, and managed respiratory collapse and severe bleeding without delay. Families are often left seeking clear answers about what happened in the delivery room and whether the response met accepted standards. If you lost a loved one due to amniotic fluid embolism in Texas, contact Hastings Law Firm for a free, confidential case review.

Compassionate Texas Medical Attorneys for Amniotic Fluid Embolism Claims
What You Should Know About AFE Malpractice Claims in Texas:
- Outcomes can be catastrophic when amniotic fluid embolism is not met with an immediate and coordinated emergency response.
- Liability often turns on failure to rescue after the first signs appear rather than on whether the embolism itself could have been prevented.
- Severe brain injury and organ injury can follow when oxygenation and circulation are not restored quickly after cardiorespiratory collapse.
- Fatal outcomes can occur when hemorrhage and clotting failure are not recognized and treated rapidly with appropriate blood products.
- Disputes commonly focus on whether early deterioration was escalated promptly and whether emergency delivery and airway management were performed without delay.
- Recovery options in Texas can be limited by strict filing time limits and other procedural requirements.
- Compensation can include medical bills, funeral costs, lost income, pain and suffering, and loss of companionship when negligence is proven.
- Case outcomes can depend on whether records such as code logs, nursing notes, anesthesia records, blood bank timestamps, and fetal monitoring strips show timely action.

A Healthcare Focused Law Firm
Losing a loved one during childbirth, or watching a mother suffer catastrophic injuries from an amniotic fluid embolism, is a devastating experience that no family should have to endure. If you are searching for answers about what happened in the delivery room, you are not alone, and your questions deserve honest, informed responses.
At Hastings Law Firm, we focus exclusively on medical malpractice litigation. Our team of attorneys, nurse consultants, and medical experts understands both the clinical and legal sides of AFE cases. As a Texas amniotic fluid embolism lawyer team, we know how to investigate whether the medical response met the standard of care and where critical breakdowns may have occurred.
If your family has been affected, we invite you to contact us for a free, confidential case evaluation. We can review what happened and explain your options.
Understanding Amniotic Fluid Embolism and Clinical Progression
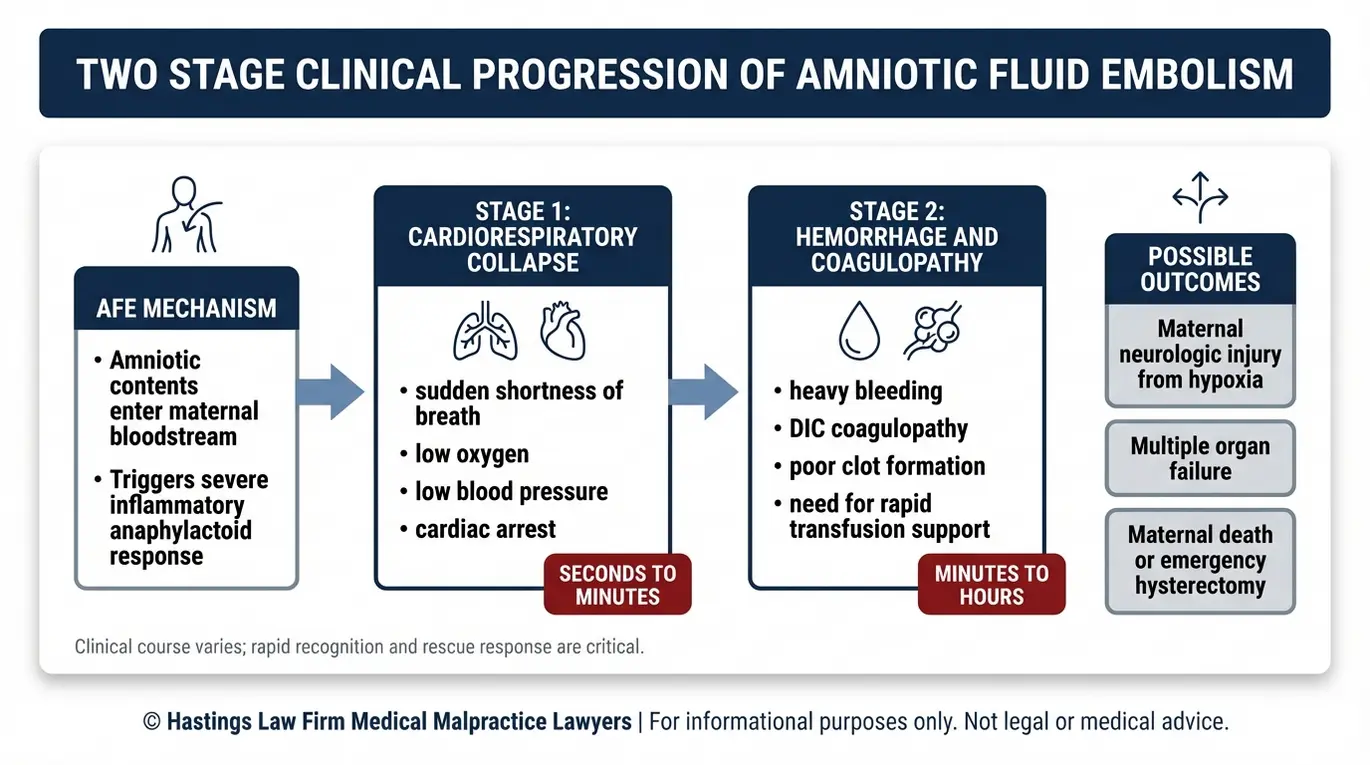
Amniotic fluid embolism (AFE), also known as Anaphylactoid Syndrome of Pregnancy (ASP), is a rare but life-threatening obstetric emergency where amniotic fluid enters the maternal bloodstream, triggering a severe allergic-like reaction that causes cardiorespiratory collapse and massive bleeding. This condition, sometimes called Anaphylactoid Syndrome of Pregnancy, requires immediate and highly specialized medical intervention.
AFE remains one of the most unpredictable complications in obstetrics. It can occur during labor, during a C-section, or shortly after delivery. According to the NCBI Bookshelf overview on Amniotic Fluid Embolism, the condition carries a mortality rate estimated between 20% and 60%, and many survivors experience lasting neurological damage or organ injury.
How AFE Progresses: The Two-Stage Cascade
Understanding the clinical progression of AFE is essential to evaluating whether the medical team responded appropriately. The condition generally unfolds in two distinct stages.
Stage 1: Cardiorespiratory Collapse
The initial phase strikes suddenly. This collapse often occurs without warning, though some patients report a sense of impending doom or aura immediately preceding the event.
The hypoxia resulting from cardiorespiratory collapse can lead to permanent brain injury within minutes if oxygenation is not restored. The mother may experience acute shortness of breath, a rapid drop in blood pressure, and respiratory failure. Within minutes, this can escalate to full cardiac arrest. The speed of this collapse is what makes AFE so dangerous and why the medical team’s immediate response is so critical.
Stage 2: Hemorrhage and Coagulopathy (DIC)
If the mother survives the initial collapse, a second wave often follows. The body’s clotting system begins to fail, a condition called disseminated intravascular coagulation (DIC), where the blood loses its ability to clot normally. DIC essentially turns the body’s clotting factors against themselves.
While clotting occurs internally, the patient bleeds profusely from IV sites, incisions, and the uterus. Controlling this hemorrhage requires rapid recognition and the immediate availability of blood products to prevent organ failure and death.
Because AFE is so rare, many labor and delivery teams may never encounter it during their careers. That rarity is precisely why these cases demand specialized medical knowledge and experienced legal analysis. Our team includes former defense attorneys and experienced hospital nurses who understand the internal clinical protocols of medical systems.
Texas AFE lawyers recognize that general practitioners may miss subtle cues in the medical records. A Texas amniotic fluid embolism lawyer must be able to work alongside qualified medical experts who can reconstruct the clinical timeline and assess whether every available intervention was deployed fast enough.
Texas law provides legal remedies for families who lose a loved one due to medical negligence under the Texas Civil Practice and Remedies Code, Chapter 71, which governs wrongful death actions in the state.
Establishing Medical Negligence in AFE Cases
Proving malpractice in AFE cases typically focuses on the medical team’s “failure to rescue,” meaning the failure to respond to the emergency according to protocol, rather than blaming them for the occurrence of the embolism itself. This distinction is central to how Texas AFE lawyers build these claims. We focus our investigation on identifying any failure to rescue that occurred during the crisis.
The “Unpreventable” Defense
Defense attorneys in AFE litigation almost always argue that the embolism itself was an unforeseeable, unavoidable event. In many instances, that is medically accurate. No one can predict when AFE will strike, and the initial event may not reflect any lapse in care.
But the legal question is not whether the AFE could have been prevented. The question is whether the medical team’s response to the emergency met the standard of care, which is the level of treatment that a reasonably competent medical professional would have provided under similar circumstances. A skilled Texas amniotic fluid embolism lawyer understands that while the event itself may be sudden, the protocol for management is well-established.
The Counter-Argument: Failure to Rescue
Liability in AFE cases often hinges on what happened in the minutes after the first signs appeared. “Failure to rescue” refers to the medical team’s inability or delay in recognizing a deteriorating patient and escalating care appropriately. When response times lag, the probability of severe maternal injuries increases exponentially. Delays in restoring circulation can lead to permanent neurological damage caused by cerebral hypoxia.
Common areas we examine include:
- Whether early warning signs like shortness of breath, sudden low blood pressure, confusion, or fetal distress were recognized and acted upon promptly
- Whether the code team was activated without delay once cardiac arrest occurred
- Whether the delivery team initiated emergency surgical intervention within the critical time window
- Whether blood products and clotting factors were ordered and administered quickly enough to address the hemorrhage phase
| Not Malpractice (Unavoidable Event) | Potential Malpractice (Failure to Rescue) |
|---|---|
| AFE occurs suddenly and without warning during otherwise normal labor | Early symptoms of respiratory distress are documented but not escalated |
| The medical team responds immediately and follows all emergency protocols | Code team activation is delayed by several minutes after cardiac arrest |
| Despite best efforts, the patient does not survive | Emergency C-section is not performed within the critical window |
| Coagulopathy develops but the massive transfusion protocol is activated promptly | Blood products are not ordered or are significantly delayed during active hemorrhage |
Proving Causation Through Differential Diagnosis
One of the most challenging aspects of AFE litigation involves differential diagnosis, the clinical process of ruling out other conditions that present similarly. AFE can mimic a pulmonary embolism, anaphylaxis, or other cardiac events. Distinguishing between these conditions is essential because each has different treatment protocols, different risk factors, and different implications for whether the outcome was preventable.
Defense teams often claim the collapse was due to a massive pulmonary embolism or primary cardiac arrhythmia to avoid liability for AFE management failures. A detailed review of the autopsy and blood panels is necessary to refute these claims.
An experienced AFE attorney in Texas works with medical experts to analyze lab results, autopsy findings, fetal monitoring strips, and the precise timing of symptom onset to establish what condition the patient was experiencing and whether the clinical team’s response was appropriate.
Urgent Maternal Warning Signs
Medical staff are trained to recognize the signs of maternal deterioration. For AFE management, the warning signs that should trigger an immediate emergency response include:
- Sudden shortness of breath or respiratory distress during labor or immediately after delivery
- Rapid drop in blood pressure (hypotension) without an identifiable cause
- Altered mental status, including confusion, agitation, or loss of consciousness
- Fetal distress on the electronic fetal monitor, which is often one of the earliest indicators that the mother’s oxygen levels are dropping
- Cardiorespiratory collapse, the sudden failure of the heart and lungs to function, which can occur within minutes of the onset of symptoms
These signs demand an immediate, coordinated response. When medical teams fail to recognize or act on these indicators, the consequences for both the mother and baby can be catastrophic.

The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Common Medical Errors in Managing AFE
Common errors in AFE management include failing to perform an immediate emergency C-section, delaying massive blood transfusion protocols during the hemorrhage phase, or failing to secure the airway during initial respiratory collapse. Consulting with AFE malpractice counsel is necessary to identifying these lapses in judgment. Each of these delays can mean the difference between life and death, or between recovery and permanent injury.
Delayed Emergency Delivery
When a mother goes into cardiac arrest during labor, medical guidelines call for a perimortem cesarean delivery (PMCD), an emergency C-section performed during or immediately after maternal cardiac arrest. In many obstetric emergencies, immediate delivery is required to protect the safety of the mother and child.
According to the NCBI Bookshelf resource on Perimortem Cesarean Delivery, this procedure should ideally be initiated within four to five minutes of arrest. The goal is twofold: to save the baby from oxygen deprivation and to improve the mother’s circulation by relieving pressure from the uterus.
When this critical window is missed, the baby faces a significantly higher risk of cerebral palsy, hypoxic brain injury, or death. The mother’s chances of survival also decrease with every passing minute.
Mismanagement of Hemorrhage
Once coagulopathy sets in during the second phase of AFE, the patient can lose massive amounts of blood in a very short period. The appropriate response is activation of a massive transfusion protocol (MTP), a pre-established hospital plan for rapidly delivering large quantities of blood products, including red blood cells, plasma, and platelets in specific ratios.
Research published by BMC Anesthesiology on transfusion and coagulation management in major obstetric haemorrhage underscores the importance of early, aggressive blood product replacement to manage emergencies. Delays in activating the MTP, or administering inadequate volumes, can lead to irreversible organ damage or maternal death.
Surgical Delays
In cases where hemorrhage cannot be controlled through transfusion and medication alone, an emergency hysterectomy may be necessary. When excessive bleeding occurs, surgical options are sometimes the only way to save a life. Hesitation or delay in making this surgical decision, particularly in the presence of conditions like placental abruption or placenta accreta, can result in continued blood loss and multiple organ failure.
Surgeons may hesitate to remove the uterus in a young patient hoping to preserve fertility, but in the context of AFE-induced DIC, this hesitation can be fatal. The speed of decision-making is a key metric we evaluate.
Monitoring Failures Before Collapse
In some AFE cases, fetal distress patterns appear on the electronic fetal monitor before the mother shows outward signs of distress. These patterns can serve as early warning signs that something is going wrong. If the nursing staff or attending physician fails to interpret or escalate those findings, the opportunity for a faster response may be lost.
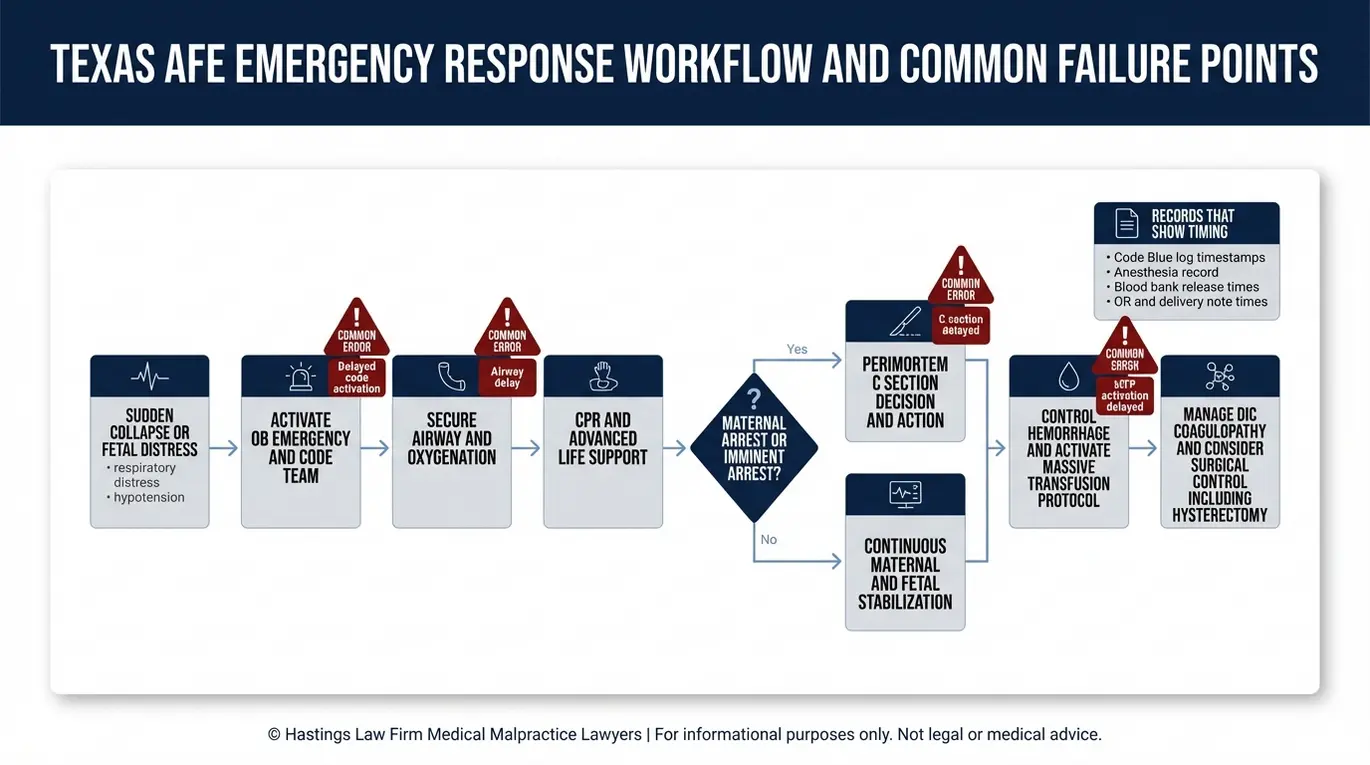
Proper AFE Emergency Response Protocol Should Include:
- Immediate activation of the code team upon recognition of cardiorespiratory collapse
- Airway management and intubation to address respiratory failure
- Initiation of perimortem C-section within four to five minutes of cardiac arrest
- Early activation of the massive transfusion protocol with balanced blood product delivery
- Continuous assessment for DIC with serial lab draws
- Surgical intervention, including hysterectomy, when hemorrhage is uncontrolled
- Transfer to ICU with critical care support for ongoing management
As a Texas amniotic fluid embolism lawyer team, we review code blue logs, nursing notes, anesthesia records, blood bank timestamps, and fetal monitoring strips to identify exactly where the protocol broke down.
Compensation and Damages for Maternal Injury or Death
Families affected by AFE-related medical negligence may recover compensation for medical bills, funeral costs, lost future income, pain and suffering, and loss of companionship through wrongful death or survival claims filed under Texas law. A knowledgeable Texas amniotic fluid embolism lawyer can maximize the recovery available under these distinct legal theories.
Wrongful Death Claims
When a mother dies as a result of negligent AFE management, Texas law allows certain family members to file a wrongful death claim. In the tragic event of maternal death, the financial impact on the family is immediate and overwhelming. The surviving spouse, children (including adult children), and parents of the deceased each have the right to seek damages for their individual losses, including:
- Loss of companionship and consortium: the emotional and relational loss experienced by the surviving family
- Lost wages and future income: the financial support the mother would have provided over her lifetime
- Mental anguish: the grief and emotional suffering caused by the loss
- Funeral and burial expenses
Survival Claims
Separate from a wrongful death action, the estate representative may also file a survival claim. A survival claim is a legal action brought on behalf of the estate for injuries sustained before death. This claim seeks compensation for the pain and suffering the mother experienced between the onset of the emergency and the time of death.
In AFE cases, where the patient may have endured cardiac arrest, emergency surgery, and prolonged ICU care, these damages can be significant. This includes compensation for the conscious physical pain and mental terror the mother likely felt as she struggled to breathe or realized her condition was deteriorating before losing consciousness.
Maternal Injury and Birth Injury Claims
Not all AFE cases result in death. Some mothers survive but sustain permanent neurological damage from oxygen deprivation during cardiac arrest. These patients may require lifelong care, rehabilitation, and assistance with daily living.
Similarly, if delays in emergency delivery caused the baby to suffer cerebral palsy or hypoxic-ischemic encephalopathy, a separate birth injury claim may be pursued. A Texas birth injury attorney can help evaluate whether the infant’s injuries were caused by preventable delays during the AFE crisis.
The lifetime costs for a child with severe brain injury can exceed several million dollars. A life care plan is often developed to project the costs of 24-hour nursing, accessible housing, and specialized therapies required over the child’s life.
Damages in these cases often include:
- Past and future medical expenses, including surgeries, therapy, and assistive equipment
- Lost earning capacity for both the mother and the child
- Pain and suffering endured by the patient
- Costs of long-term nursing care or residential support
Texas Laws Affecting AFE Malpractice Litigation
Texas law imposes a strict two-year statute of limitations for filing medical malpractice claims and requires a specialized expert report to be served within 120 days of the date each defendant’s original answer is filed. Legal time limits apply to all medical claims in Texas, and we ensure every requirement of Chapter 74 is met early in the process.
Statute of Limitations
Under Texas law, families generally have two years from the date of the negligent act to file a medical malpractice lawsuit. This usually starts on the date of birth or death. There are limited exceptions, such as the discovery rule for injuries that are not immediately apparent.
Claims involving minors under the age of 12 may have a longer filing window. These claims allow the child until their 14th birthday to file or have a claim filed on their behalf, but parents should not rely on this extension. Evidence can disappear and memories fade, so securing legal representation early is the safest course.
Chapter 74 Expert Report Requirement
Texas Civil Practice and Remedies Code Chapter 74 requires plaintiffs in medical malpractice cases to serve a written expert report within 120 days of the date each defendant’s original answer is filed. This report must be authored by a qualified physician, such as an OB-GYN or Maternal-Fetal Medicine specialist, and must specifically address three things: the applicable standard of care, how it was breached, and how that breach caused the injury or death. Failure to serve this report on time results in mandatory dismissal of the case.
This report acts as a gatekeeper. If the report is deemed insufficient by the court, the judge must dismiss the case and may even order the plaintiff to pay the doctor’s legal fees.
This high procedural hurdle makes it imperative to retain counsel who has access to reputable medical experts immediately. Working with an experienced Texas amniotic fluid embolism lawyer matters early in the process for these reasons. The expert report requirement means the medical investigation must begin immediately, not months after filing.
Caps on Non-Economic Damages
Texas also imposes caps on non-economic damages in medical malpractice cases, which limit recovery for pain and suffering and loss of companionship. Economic damages, including medical bills, lost wages, and future care costs, are not subject to any cap.
Contact the Texas Birth Injury Attorneys at Hastings Law Firm Today for Help
While amniotic fluid embolism is an unpredictable event, the medical response that follows must be competent, timely, and aggressive. When it is not, families deserve answers and accountability.
At Hastings Law Firm, we understand that your search for a Texas amniotic fluid embolism lawyer is about more than compensation. It is about learning the truth of what happened and working to prevent the same failures from affecting another family. Our founder, board-certified attorney Tommy Hastings, is recognized as a leading authority on medical malpractice and prepares every case to be trial-ready from the start.
We handle AFE malpractice cases on a contingency fee basis, which means you pay no attorney fees or costs unless we secure a recovery on your behalf.
If you have lost a loved one or a family member has suffered serious injury following an amniotic fluid embolism, contact our Texas AFE attorneys today for a free, confidential case evaluation. Let us help you find the answers you deserve.
Frequently Asked Questions About Amniotic Fluid Embolism in Texas

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
