

Texas Altered Hospital Records Lawyer
Written by: Hastings Law Firm | Reviewed by: Brady D. Williams | Updated: May 6, 2026
Suspected falsification of medical records can deepen the harm of a medical injury by undermining trust and obscuring what really happened. Altered charts can hide mistakes, shift blame, and make it harder to understand whether care met professional standards, especially when only a static printout is provided instead of the underlying electronic data. Knowing how electronic records track edits and access can clarify what evidence may exist and why it matters. If you or a loved one were harmed or worse due to altered hospital records in Texas, contact Hastings Law Firm for a free, confidential case review.

Trusted Texas Medical Attorneys for Falsified Medical Records Malpractice Claims
What You Should Know About Falsified Medical Records Malpractice Claims in Texas:
- Accountability can be harder to establish when a hospital provides only a PDF record because it can hide audit trail data and prior versions.
- Proof of record tampering can change the seriousness of a malpractice dispute because it can shift the focus from negligence to fraud or gross negligence.
- Recovery can be affected when a court allows an inference against the defense after evidence is materially altered or destroyed.
- Options can narrow if digital evidence is overwritten or purged, making early preservation of electronic data consequential.
- Credibility can collapse when audit trail metadata conflicts with a provider account of when care occurred.
- Compensation can expand when record falsification supports exemplary damages in addition to other damages.
- Clarity can depend on obtaining records in native format because it preserves user identifiers, timestamps, and version history.
- Disputes can be resolved by comparing electronic entries with other sources such as radiology timestamps or pharmacy records.
- Emotional harm can be compounded when a provider is perceived to have concealed mistakes through altered documentation.
- Access to personal health information can be central to evaluating concerns about altered records under federal privacy rules.

A Healthcare Focused Law Firm
When you suspect that a hospital or doctor changed your medical records to hide a mistake, the sense of betrayal can be overwhelming. You already know something went wrong with your care. Now you may be facing the possibility that the very records meant to document the truth have been manipulated against you. That suspicion is valid, and you deserve to have it investigated by someone who knows exactly where to look.
At Hastings Law Firm, our team includes in-house nurses and former defense attorneys who spent years working inside the hospital systems we now hold accountable. We understand how records are created, how they can be changed, and how to uncover the digital evidence that proves it. If you need a Texas Altered Hospital Records Lawyer, we are ready to review what happened and explain your options in a free, confidential consultation.
Investigating Electronic Medical Record Tampering and Forgery
Falsifying medical records is a deliberate attempt to hide malpractice by altering, deleting, or fabricating patient data. This often occurs through “late entries” made after a patient suffers harm, or by suppressing the digital metadata that proves when a change was actually made. Detecting these alterations is critical to preventing the spoliation of evidence, which is the destruction or material alteration of proof, and securing the justice you deserve.
To understand how this works, you need to understand how modern hospital charting operates. Most hospitals use an Electronic Medical Record system, commonly called an EMR or EHR, which is the digital platform where every note, order, vital sign, and lab result is documented. Systems like Epic and Cerner do more than store information. They create what amounts to a digital fingerprint every time a record is opened, viewed, edited, or deleted.
This fingerprint is called an audit trail, a permanent log embedded in the system that tracks who accessed a patient’s chart, what they changed, and precisely when they did it. The Office of the National Coordinator for Health Information Technology (HealthIT.gov) recognizes audit logging as a core certification requirement for health IT systems. That means the data exists, stored deep within the system’s architecture. The question is whether anyone demands to see it, or if it remains hidden behind the PDF printout.
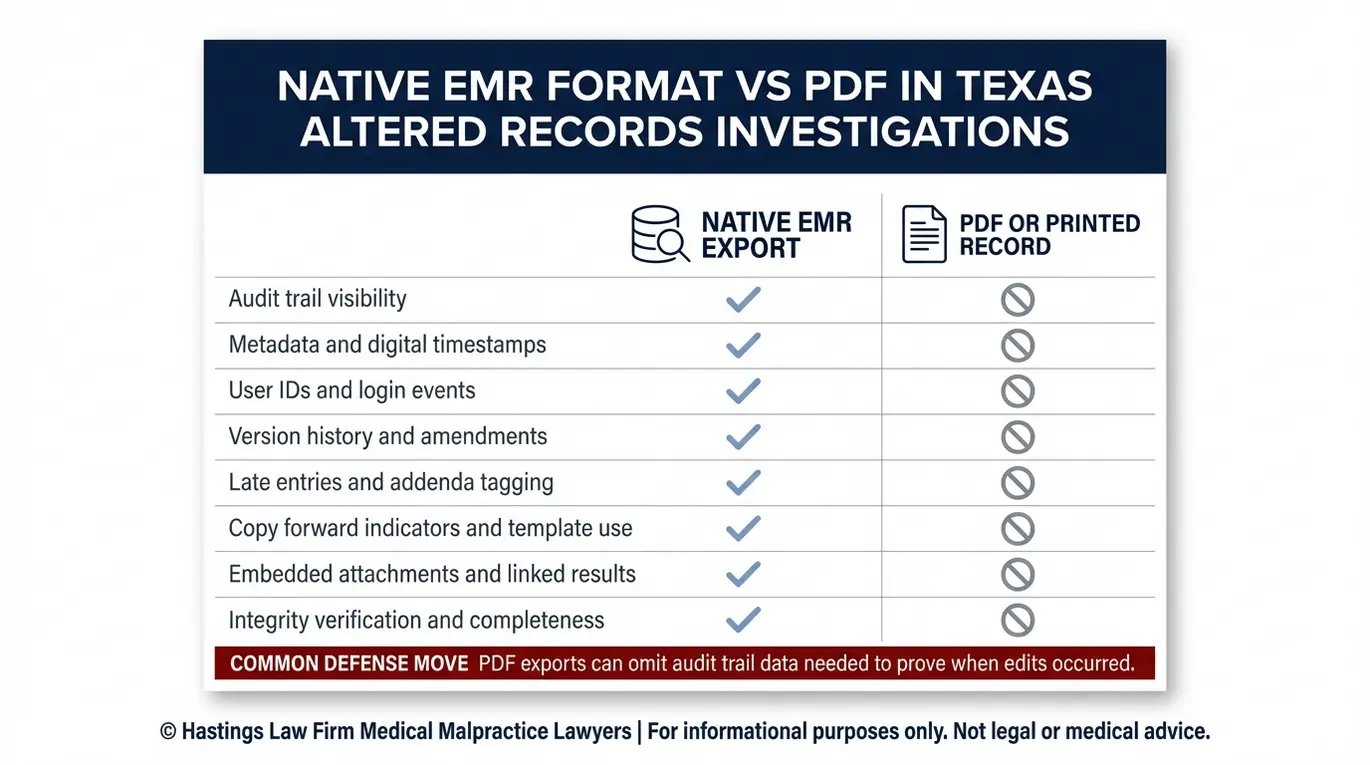
Here is the problem: when hospitals respond to records requests, they almost always send a PDF printout. A PDF is a flat, static file that strips away the audit trail, metadata, digital timestamps, and version history. It shows what the record says now, but it hides what it said before and when it was changed.
That is why a Texas altered medical records lawyer will demand the records in native format, which is the original database export directly from the EMR system. Native format preserves every layer of data, including user login IDs, edit timestamps, and the full history of changes made to each entry. This format is essential because it is the only way to see the underlying data structure.
Without it, you are essentially looking at a photograph of the chart rather than the chart itself, missing the context needed to prove tampering. When our team reviews native format records, we look for specific red flags of tampering:
- Late entries made days or weeks after an adverse event that conveniently fill in gaps in the original documentation
- Identical timestamps on multiple complex procedures, suggesting notes were batch-entered after the fact
- Generic “copy-forward” text that does not match the patient’s actual condition or clinical course
- Missing segments or unexplained gaps in the audit trail where entries appear to have been deleted
- Altered or overwritten medication orders that differ from pharmacy dispensing records
These patterns do not always mean fraud on their own, but they raise serious questions that deserve forensic investigation. An attorney for falsified hospital records will know how to interpret these discrepancies and use them to build your case.
Chart Creep and the Danger of Copy-Forward Errors
One of the more insidious forms of record manipulation is something called chart creep. This occurs within Electronic Medical Record (EMR) systems when data is recycled from previous patient encounters. This happens when a provider uses the copy-forward function, essentially a copy-and-paste tool built into most EMR systems, to duplicate a previous note into a new entry.
The provider may change a few words or leave the note entirely unedited. Over time, this creates a medical record that looks thorough on paper but is actually recycled text that does not reflect what happened during a specific visit or procedure. A patient’s chart may show a detailed physical exam on a day the doctor barely entered the room.
It may reflect assessments that were never performed or findings that belong to a completely different date. Chart creep can mask a diagnosis error, hide a failure to examine, or create false evidence that a provider met the standard of care when they actually committed medical negligence. Our in-house nursing staff is trained to spot these inconsistencies by cross-referencing charted notes against nursing logs, lab results, and radiology timestamps.
Is It Illegal to Alter Medical Records in Texas?
Yes. Altering medical records with the intent to deceive or hide negligence is illegal and creates significant civil liability. Our founder, Tommy Hastings, is Board Certified in Personal Injury Trial Law by the Texas Board of Legal Specialization, a distinction held by fewer than 2% of attorneys in the state. In a malpractice lawsuit, proven alteration can lead to spoliation sanctions, where the court instructs the jury that it may infer the missing or destroyed evidence would have been unfavorable to the defense.
Texas law addresses falsification from both the criminal and civil side. Under the Texas Penal Code Chapter 37, tampering with records or evidence can constitute a criminal offense, and such actions may also trigger disciplinary action by the Texas Medical Board. But for patients, the civil liability is where the real impact lies.
When a standard medical malpractice case involves altered records, it transforms. What might have been a negligence claim based on a medical error now becomes a case involving fraud and potential gross negligence. Juries tend to react strongly to dishonesty. The original mistake may have been understandable under the circumstances.
The cover-up tells the jury that the provider knew something went wrong and chose to hide it rather than own it. That reaction can open the door to punitive damages, which are designed to punish especially harmful conduct and deter others from doing the same. We distinguish between legitimate corrections and fraudulent alterations.
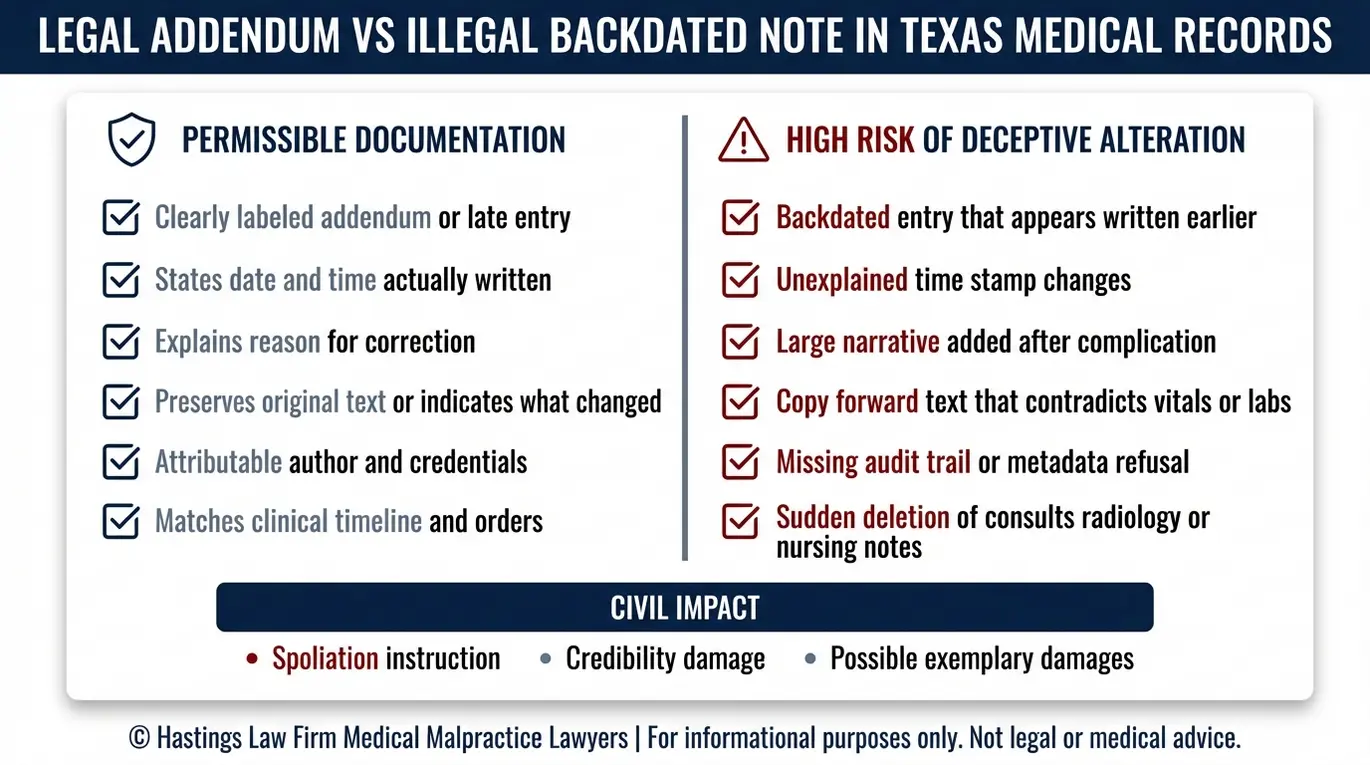
Healthcare providers are allowed to make corrections to the medical record. A proper correction is called an addendum or late entry, a clearly marked note that identifies the original author, states the date and time of the addition, and explains why the change was made. The original entry remains visible and unaltered.
A fraudulent alteration, by contrast, is a backdated note designed to look like it was written at the time of care. It may overwrite the original entry, omit the author’s identity, or lack any indication that it was added after the fact. A lawyer for altered medical charts in Texas knows how to distinguish one from the other using audit trail data and forensic analysis.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Texas courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Steps to Take If You Suspect Your Records Were Falsified
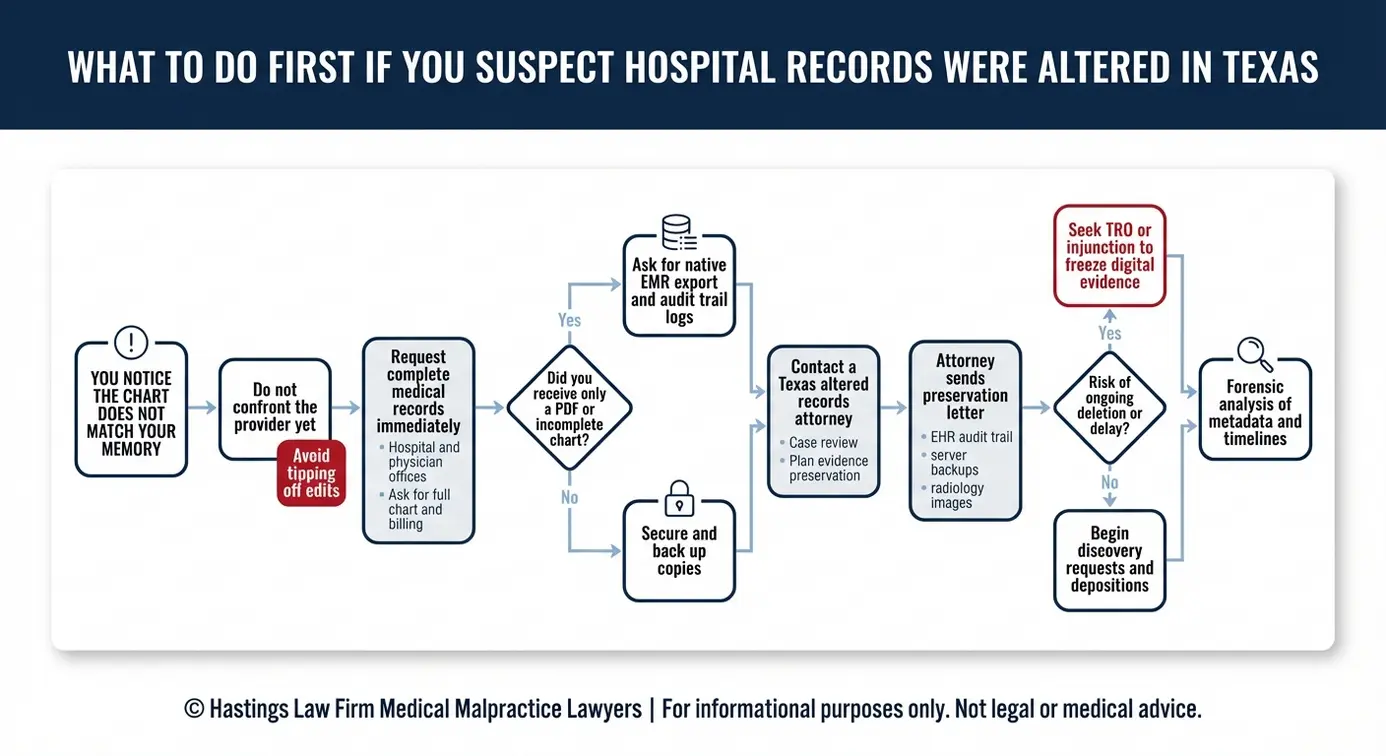
If you suspect tampering, do not confront the doctor or hospital directly. Request a complete copy of your medical records as soon as possible to preserve the current version, then contact a specialized attorney who can issue a formal preservation of evidence letter to prevent further changes or deletion.
Here is why that sequence matters, and what each step involves:
Do not alert the provider. Your instinct may be to demand answers from the doctor or hospital administrator immediately. However, alerting them to your suspicions gives them an opportunity to cover their tracks. If a provider knows you are onto them, they may attempt to scrub the metadata or delete the “late entry” tags before you have secured a copy. Silence, at this stage, is a strategic advantage that protects the integrity of your potential case.
Request your records immediately. Under federal law (HIPAA), you have the right to obtain a copy of your medical records. Submit a written request to the hospital’s medical records department. Ask for the complete record, including nursing notes, physician orders, operative reports, lab results, and radiology images. Be specific that you want the “legal medical record.” Obtaining this “clean” copy before formal litigation begins provides an important baseline for comparison.
Contact a Texas Altered Hospital Records Lawyer. Once an attorney is involved, several things can happen quickly to protect the evidence you need:
- Your attorney can send a preservation of evidence letter directly to the hospital, putting them on legal notice that records must not be altered, deleted, or overwritten
- If there is reason to believe records are actively being destroyed, your attorney can seek a Temporary Restraining Order (TRO) from the court, compelling the hospital to freeze its systems
- Your attorney can file formal written discovery requests demanding the records in native format, including the full audit trail and metadata
Each of these steps locks the evidence in place before it can be changed further. While the formal discovery process will eventually allow us to subpoena the full system data, these preliminary protective measures are important to ensure that the data still exists when that time comes.
Using Injunctions to Preserve Digital Evidence
In urgent situations, waiting for the normal discovery process is not an option. A court-ordered injunction is a legal tool used to protect digital medical files from being overwritten. This legal order prevents hospitals from deleting or overwriting sensitive electronic data during an investigation.
EMR systems can be configured to purge old audit data, and server backups may be overwritten on a rolling schedule. When digital evidence is at risk of disappearing, a court-ordered injunction or TRO can force the hospital to freeze its server backups and preserve every version of the record as it currently exists.
This kind of immediate legal action requires an attorney who understands both the technology and the procedural rules. Our team has experience filing these emergency motions and working with IT professionals to ensure the right data is captured before it is gone.
Proving Malpractice Through Forensic Analysis
Proving alteration requires comparing the printed record against the backend metadata. Our team works with forensic experts to identify discrepancies in timestamps, user logins, and version history that reveal when a critical entry was modified or deleted.
The process starts with obtaining the native EMR data through formal discovery. Once we have that data, our forensic document experts and in-house medical staff examine it layer by layer. They compare what the hospital provided in its initial PDF against what the system’s metadata actually shows. Discrepancies between these two versions can be powerful evidence of tampering.
Even in a digital world, physical documents still matter. Consent forms, bedside flow sheets, and handwritten physician orders may contain evidence that contradicts the electronic record. A handwriting expert can analyze whether signatures were added after the fact or whether entries were written by someone other than the listed author.
Depositions and cross-examination are where this evidence becomes most effective. When a skilled attorney confronts a provider with audit trail data during a deposition, the results can be decisive. For example, if a physician testifies that they assessed a patient at 2:00 PM, but the EMR metadata shows they were logged into a terminal on a different floor at that time, the contradiction speaks for itself.
Radiology images, lab results, and operative reports deserve special attention. These records carry their own timestamps and are often stored in separate systems from the main EMR. If imaging results were available hours before a provider claims to have reviewed them, that gap in the record can establish both the malpractice and the attempt to conceal it.
Under HIPAA regulations, as outlined by the Assistant Secretary for Technology Policy (HealthIT.gov), healthcare providers are required to maintain the integrity and confidentiality of patient records. When those obligations are violated, a falsified medical records attorney can use the breach itself as evidence of wrongdoing. As a Texas Altered Hospital Records Lawyer, our firm has the forensic resources and medical knowledge to build these cases from the ground up.
Compensation for Victims of Medical Fraud and Negligence
Patients harmed by malpractice involving altered records may be entitled to compensation for medical bills, lost wages, and pain and suffering. Evidence of record falsification can also support a claim for exemplary (punitive) damages designed to punish the wrongdoer and deter similar conduct.
The damages in these cases generally fall into three categories:
Economic damages cover the financial losses you can document. These include past and future medical expenses, rehabilitation costs, lost wages, and diminished earning capacity. When malpractice causes a permanent injury or disability, the future cost of care can be substantial, and we work with medical economists to calculate those figures accurately.
Non-economic damages address the harm that does not come with a receipt. Pain, suffering, mental anguish, and loss of enjoyment of life all fall into this category. In cases involving falsified records, the emotional toll is often compounded by the betrayal of trust.
Learning that a provider not only made a mistake but actively tried to hide it can cause lasting psychological harm. The Texas Civil Practice and Remedies Code Chapter 74 does impose caps on non-economic damages in medical malpractice cases, which is something your attorney will factor into your case strategy.
Punitive (exemplary) damages are not available in every malpractice case, but record falsification can change that calculation. If the evidence supports a finding of fraud, malice, or gross negligence, punitive damages may become recoverable. Even when a case settles before trial, the threat of punitive exposure gives your Texas altered medical records malpractice lawyer a significant advantage in negotiations, potentially increasing the settlement value of your claim.
You also have the right to access your own health information under federal law. The U.S. Department of Health and Human Services outlines your rights under HIPAA to obtain copies of your records, which is often the first step in building your case. In wrongful death cases, surviving family members may pursue these same categories of damages on behalf of their loved one.
Contact the Texas Hospital Malpractice Attorneys at Hastings Law Firm Today for Help
If you believe a hospital or doctor altered your records to cover up a mistake, you are dealing with a situation that requires a legal team with specific forensic and medical resources. Our firm was founded by Tommy Hastings in 2005 to exclusively handle medical malpractice and provide a voice to patients across Texas. We understand the technical and emotional challenges of proving hospital record tampering.
Our team, which includes in-house nurses, former defense attorneys, and board-certified trial lawyer Tommy Hastings, knows how to obtain, analyze, and present the digital evidence that exposes record tampering. We operate on a contingency fee basis, which means you pay no attorney fees or costs unless we recover compensation for you. Our founder, Tommy Hastings, is an inductee into ABOTA, an organization for elite trial lawyers, reflecting his status as one of the state’s leading authorities on medical malpractice.
If you need a Texas Altered Hospital Records Lawyer, contact us today for a free, confidential case evaluation. Let us help you find the answers you deserve.
Frequently Asked Questions About Altered Hospital Records in Texas

Key Altered Hospital Records Terms:
- Electronic medical record (EMR/EHR)
- A digital version of a patient’s medical chart that stores health information in a computer system. In a malpractice case, EMR systems like Epic or Cerner are critical because they automatically track who accessed or changed the record and when, creating a trail that can reveal if a doctor or hospital altered notes after an injury occurred.
- Native format (vs. PDF export)
- The original file format in which an electronic medical record is stored by the hospital’s computer system, containing hidden data like edit history and timestamps. Hospitals often provide records as PDF exports, which strip out this hidden information, making it harder to detect tampering. Attorneys request native format files to see the complete digital fingerprint of the record.
- Audit trail (EMR access/change log)
- An automatic record kept by electronic medical record systems that logs every time someone opens, views, edits, or deletes a patient’s chart, including the user’s identity and the exact time of access. In malpractice cases involving suspected tampering, the audit trail acts as digital evidence showing whether a doctor added or changed notes after a patient was harmed.
- Metadata (including digital timestamps and user IDs)
- Hidden information embedded in electronic files that reveals when a document was created, modified, or accessed, and by whom. In medical malpractice cases, metadata can prove that a doctor backdated a note or added critical information to a chart days or weeks after the fact to cover up a mistake.
- Late entry
- A note added to a medical record after the date of the patient encounter it describes, but clearly labeled as being written later. A legitimate late entry is marked with the actual date it was written and explains why it was delayed. If a doctor tries to make a late entry look like it was written at the time of treatment without disclosure, that can be evidence of fraud in a malpractice case.
- Addendum
- An addition or correction made to an existing medical record after it was originally completed, properly dated with the current date and labeled as supplemental information. Unlike fraudulent alterations, a lawful addendum does not erase or hide the original entry and clearly shows it was added later, preserving the integrity of the medical record.
- Chart creep
- The practice of medical records gradually becoming filled with outdated, inaccurate, or irrelevant information that gets repeatedly copied from one visit to the next. This often happens when healthcare providers use copy-forward features in electronic systems, causing old symptoms or findings to appear in current notes even though they no longer apply, which can lead to dangerous errors or obscure what actually happened during a specific visit in a malpractice case.
- Copy-forward (copy/paste charting)
- A shortcut feature in electronic medical record systems that allows doctors and nurses to copy text from a previous note and paste it into a current one. While this saves time, it can create misleading records when generic or outdated information is carried forward without being updated to reflect the patient’s actual condition at the time, making it difficult to determine what the provider truly observed or did during a visit when investigating malpractice.
- Texas Penal Code Chapter 37 Perjury and Other Falsification | Texas Legislature Online
- Texas Civil Practice and Remedies Code Chapter 74 | Texas Legislature Online
- Individuals’ Right under HIPAA to Access their Health Information | HHS gov
- Auditing actions on health information | HealthIT.gov
- HIPAA for Providers | ASTP Assistant Secretary for Technology Policy
- Civil Practice and Remedies Code Chapter 74 | Texas Legislature Online
Get Answers Today
If you think that medical negligence, a dangerous drug, or a failed medical product caused harm to you or someone you love, our team is standing by to offer guidance. We’ll explain your options under current laws and help you move forward with clarity and understanding. Case reviews are free and 100% confidential.
