

Arizona VBAC Complications Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Trial of labor after cesarean can be safe when proper safeguards are in place, but breakdowns in monitoring, staffing readiness, and timely decision making can lead to catastrophic outcomes for a mother or baby. Serious VBAC complications described here include uterine rupture, oxygen deprivation injuries, uncontrolled hemorrhage, and emergency hysterectomy. Concerns often center on missed warning signs, delayed emergency cesarean delivery, and incomplete informed consent about specific risks. If you or your child were harmed or worse due to VBAC complications in Phoenix, Arizona, contact Hastings Law Firm for a free, confidential case review.

Compassionate Arizona Medical Attorneys for Trial of Labor After Cesarean Malpractice Claims
What You Should Know About Trial of Labor After Cesarean Malpractice Claims in Arizona:
- Permanent brain injury or death can result when uterine rupture is not treated as an immediate emergency requiring rapid delivery.
- Life altering outcomes can follow when fetal heart rate changes and other warning signs are missed, ignored, or misread during TOLAC.
- Severe maternal harm can occur when hemorrhage is not controlled quickly, including the need for an emergency hysterectomy.
- Recovery options can be affected when informed consent discussions are not detailed and documented for the specific patient history.
- Preventable injury risk can increase when a hospital is not prepared to perform an emergency cesarean immediately with anesthesia and surgical staff ready.
- The severity of a newborn injury can hinge on delays between the first documented warning sign and delivery.
- Rupture risk can rise when labor is induced or augmented during VBAC, especially when contractions become overly frequent.
- Serious complications can be linked to the use of specific induction agents in patients with a prior cesarean scar.
- Case clarity can depend on whether fetal monitoring data, staffing logs, pharmacy records, and nursing documentation are complete and consistent.
- Available legal options can narrow when filing deadlines are missed, and key hospital records may disappear over time.

A Healthcare Focused Law Firm
When a vaginal birth after cesarean (VBAC), an attempt to deliver vaginally after a prior C-section, results in serious harm to you or your baby, the confusion and grief can feel overwhelming. You trusted your medical team to keep you safe, and now you may be left with more questions than answers about what went wrong.
You are not alone, and your instinct that something should have been handled differently deserves to be taken seriously. As an Arizona VBAC complications lawyer, Hastings Law Firm focuses exclusively on medical malpractice. Our team of attorneys, nurse consultants, and former defense counsel understands both the medicine and the law behind these cases.
If you or your child were injured during an attempted VBAC, we can review what happened and explain your legal options at no cost and with no obligation.
Proving Medical Negligence in Failed VBAC Procedures
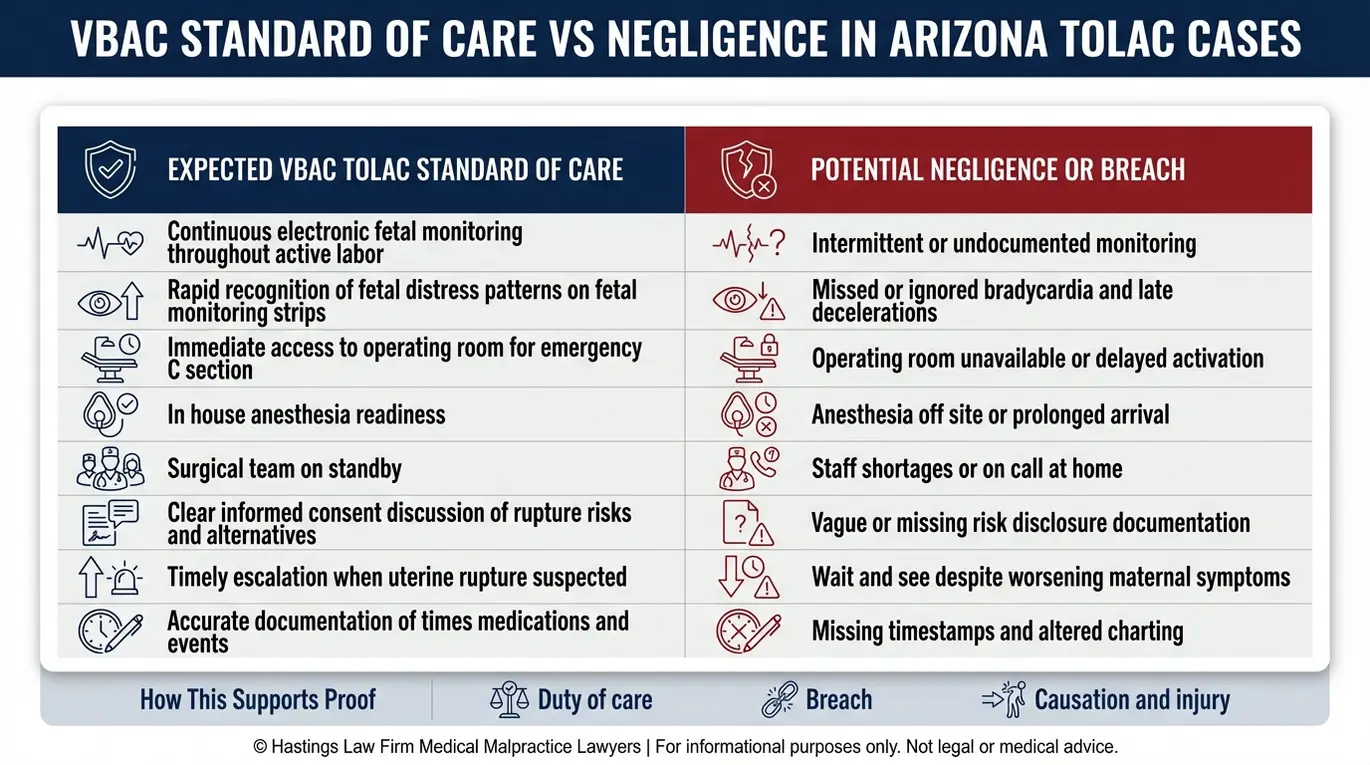
Negligence in VBAC cases is often established by showing the medical team failed to continuously monitor fetal heart rates or delayed an emergency C-section despite clear signs of uterine distress. In Arizona, a medical malpractice claim requires proof that a healthcare provider’s care fell below the accepted standard of care. This represents the level of treatment a reasonably competent OB-GYN would provide under similar circumstances, per Arizona Revised Statutes § 12-563.
A trial of labor after cesarean (TOLAC), the medical term for the attempt itself before a successful vaginal delivery is confirmed, carries well-documented risks. Because of those risks, the standard of care requires specific safeguards be in place before and throughout labor. Hospitals must be equipped to handle surgical emergencies instantly, not just quickly, ensuring that an operating room and surgical team are standing by. When those safeguards break down or providers become complacent, serious injuries can follow.
Common failures we investigate in TOLAC cases include:
- Failure to use electronic fetal monitoring (EFM), continuous tracking of the baby’s heart rate and the mother’s contractions, throughout the entire labor
- Ignoring or misreading fetal monitoring strips that showed signs of fetal distress
- Lack of immediately available anesthesia or surgical staff for an emergency cesarean section
- Failure to obtain proper informed consent, meaning the doctor did not fully explain the specific risks of uterine rupture, hemorrhage, or other VBAC-related dangers compared to a planned repeat C-section
- Continuing labor despite worsening maternal or fetal signs that called for urgent intervention
Each of these failures can independently support a medical negligence claim. Informed consent is particularly important; the conversation must be detailed and documented. A physician cannot simply mention risks generally; they must explain how those risks apply to the specific patient’s medical history. If a mother is not given the full picture, she cannot make a truly informed choice about her body and her baby’s safety.
Our Phoenix legal team reviews medical records, staffing logs, and fetal monitoring data to reconstruct what happened. Our team includes former hospital defense attorneys and nurses who provide insider insight into hospital protocols and charting inconsistencies. An experienced Arizona birth injury attorney knows that missing logs or inconsistent monitoring strips are often the first clues of malpractice.
Identifying Uterine Rupture and Critical Delays in Care
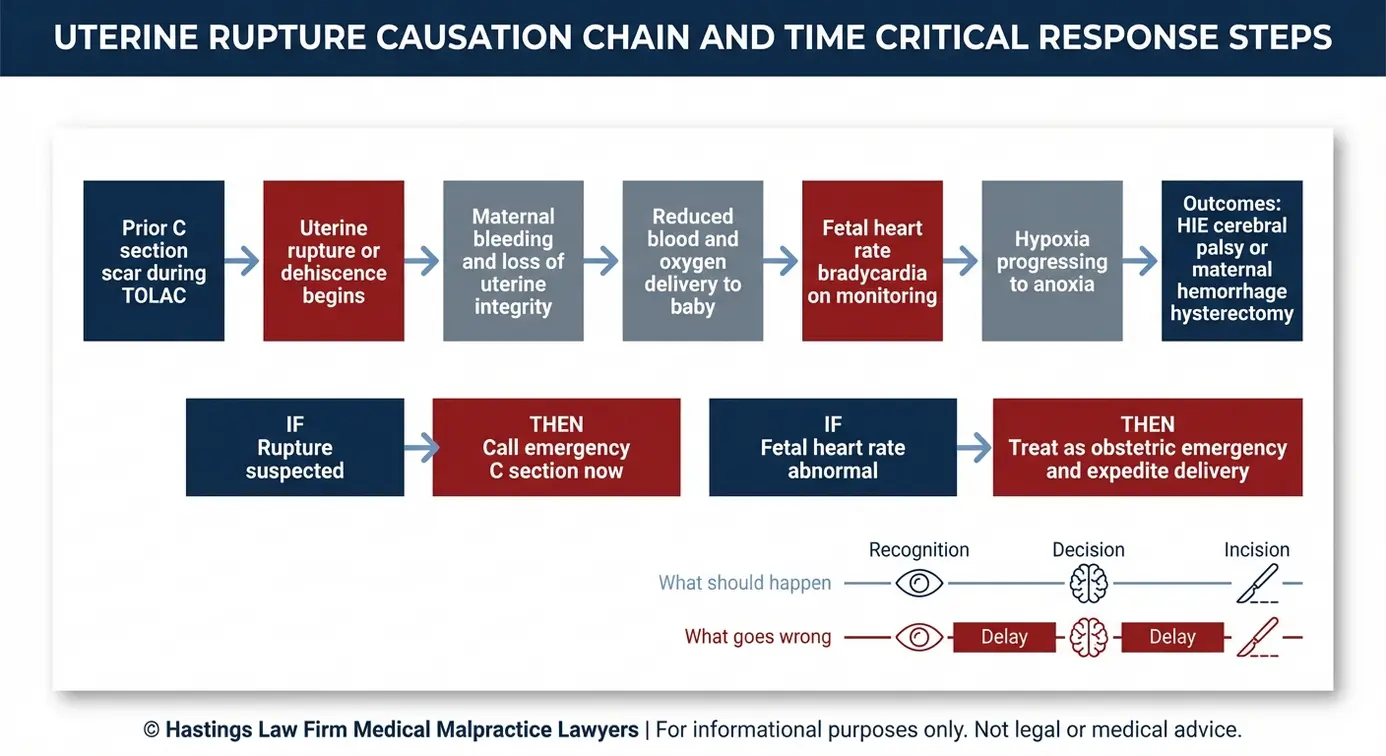
Uterine rupture is a catastrophic complication where the scar from a prior C-section tears open during labor, and it requires delivery within minutes to prevent permanent brain damage or death. This is distinct from uterine dehiscence, an incomplete separation of the scar with the outer layer of the uterus (serosa) remaining intact. A full rupture, however, can sever the blood supply to the baby, leading to hypoxia (oxygen deprivation), anoxia (complete loss of oxygen), or birth asphyxia, any of which can cause lasting neurological injury.
The Merck Manual Professional Edition on Uterine Rupture describes this as a life-threatening emergency. Uterine rupture occurs when the uterine wall tears, often at a previous surgical scar, which can compromise the baby’s oxygen supply and cause hemorrhage for the mother. For the mother, uncontrolled hemorrhage may require an emergency hysterectomy. For the baby, even a few minutes of oxygen loss can result in hypoxic ischemic encephalopathy (HIE), a type of brain injury caused by interrupted blood and oxygen flow, or cerebral palsy.
Warning signs of uterine rupture that the care team should recognize immediately:
- Sudden, severe abdominal pain, especially between contractions
- An abrupt drop in fetal heart rate (bradycardia)
- Loss of fetal heart rate tracing on the monitor
- Maternal signs of shock, including rapidly falling blood pressure and rising heart rate
- Vaginal bleeding or a change in the shape of the uterus
- Sudden cessation of contractions
When these signs appear, every minute matters. A uterine rupture lawyer at Hastings Law Firm examines the timeline between the first documented warning sign and the moment the baby was delivered to determine whether the response was fast enough.
The “Decision-to-Incision” Timeline
The American College of Obstetricians and Gynecologists (ACOG) has long referenced a 30-minute benchmark as the maximum acceptable time from the decision to perform an emergency C-section to the first surgical incision. But in a true uterine rupture, that window is far too generous. Clinical evidence suggests that once a rupture occurs, the baby may need to be delivered within 5 to 10 minutes to avoid birth asphyxia and permanent injury like HIE.
The decision-to-incision interval, the measured time between when a physician orders the cesarean and when the incision is made, is one of the most important pieces of evidence we analyze. This emergency C-section timing must be optimized for TOLAC patients. If the hospital did not have a surgical team and anesthesiologist physically present and ready, that delay can be the difference between a healthy delivery and a life-altering injury.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Risks of Inducing Labor During a VBAC
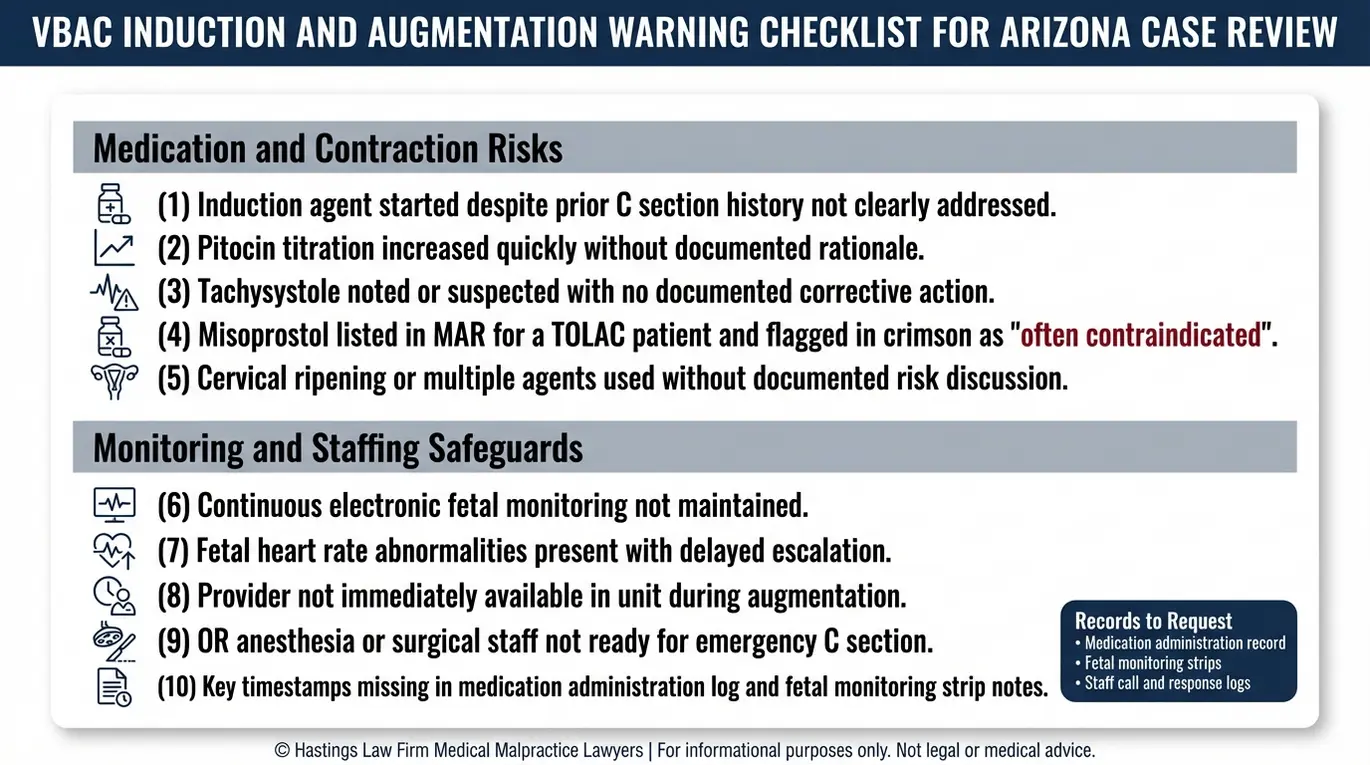
Using chemical induction agents during a VBAC can aggressively stimulate contractions, significantly increasing the risk of the uterus rupturing at the previous scar site. Labor induction agents are medications used to start or strengthen uterine contractions. This is why the decision to induce or augment labor in a TOLAC patient requires careful medical judgment and close monitoring.
Drugs like Pitocin (synthetic oxytocin) or prostaglandins like Cervadil are sometimes used for these purposes, but they increase the intensity of uterine contractions in a uterus that already has a vulnerable scar. Research published in a PubMed Central study on risk factors for uterine rupture during TOLAC confirms the elevated rupture risk associated with these agents.
Because induction forces the uterus to work harder than it might naturally, the strain on the scar tissue is intense. Medical teams must be hyper-vigilant during this process. Any sign of hyperstimulation (too many contractions in a short period) requires immediate action to reduce the drug dosage or stop it entirely. Failing to react to these warning signs is a frequent cause of preventable rupture.
Misoprostol (also known by the brand name Cytotec) poses an even greater concern. This prostaglandin drug is widely considered contraindicated for patients with a prior cesarean scar because it can cause intense, difficult-to-control contractions. A separate PubMed Central study on patient decision-making in TOLAC versus repeat cesarean delivery highlights how important full risk disclosure is before labor begins.
We review pharmacy records, physician orders, and nursing documentation to determine whether induction or augmentation drugs were used appropriately. We evaluate whether the dosing followed accepted protocols and whether monitoring was increased to match the added risk.
Contact the Arizona Birth Injury Attorneys at Hastings Law Firm Today for Help
If your baby was harmed during an attempted VBAC, or if you suffered a uterine rupture or other serious complication that you believe could have been prevented, you deserve clear answers about what happened and why.
Hastings Law Firm has a Phoenix office and a team built specifically for cases like these. Our founder, Tommy Hastings, is a board-certified trial lawyer with over 20 years of experience in medical negligence law. Our in-house medical staff and former defense attorneys know how to identify where the standard of care broke down and how to hold the responsible parties accountable.
As an Arizona VBAC complications lawyer, we handle every case on a contingency fee basis, which means you pay no attorney fees unless we recover compensation for you. Contact us today for a free, confidential case evaluation. Let us help you find the answers you and your family deserve.
Frequently Asked Questions About VBAC Complications in Arizona

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
