

Arizona Rh Incompatibility Birth Injury Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Rh incompatibility is a preventable pregnancy complication that can cause severe anemia and dangerous newborn complications when routine screening and timely treatment are missed. When an Rh negative mother becomes sensitized, antibodies can cross the placenta and damage a baby’s red blood cells, leading to lasting harm. Clear medical protocols exist for blood type testing, antibody screening, and Rh immune globulin dosing, and breakdowns in care can have permanent consequences for a child and family. If you or a loved one were harmed or worse due to Rh incompatibility birth injury in Arizona, contact Hastings Law Firm for a free, confidential case review.

Compassionate Legal Advocacy for Preventable Birth Injuries in Arizona
What You Should Know About Infant Rh Disease Claims in Arizona:
- Lifelong medical and caregiving needs can follow when Rh incompatibility is not prevented or managed and brain injury or permanent disability results.
- The most severe outcomes can occur when severe fetal anemia progresses to hydrops fetalis and is not treated aggressively.
- Preventable harm is more likely when routine prenatal blood type testing and antibody screening are missed early in pregnancy.
- Serious newborn complications can follow when Rh immune globulin is not given at the recommended times and sensitization occurs.
- Hidden exposure events can create major risk when Rh immune globulin is not given after pregnancy related bleeding, trauma, or invasive procedures.
- Treatment options can narrow when fetal anemia is not recognized and escalated care such as transfusion or early delivery is delayed.
- Disputes about responsibility can broaden when laboratory or blood bank errors affect blood typing or antibody test reporting.
- Clear documentation gaps can become central when records do not show whether Rh immune globulin was administered or antibody results were followed.
- Long term compensation issues can be driven by life care planning needs when a child requires ongoing therapy, specialized education, or adaptive equipment.
- Wrongful death damages may be pursued when severe hydrops fetalis leads to stillbirth or neonatal death.

A Healthcare Focused Law Firm
When a baby is harmed by a condition that routine prenatal care should have caught and prevented, the grief and confusion can feel overwhelming. Rh incompatibility is one of those conditions. With proper screening and timely treatment, the serious complications it causes are almost entirely avoidable. When a provider fails to follow well-established protocols, the consequences for an infant can be devastating and permanent.
If your child suffered a birth injury that you believe was connected to Rh disease or a missed RhoGAM injection, you are not wrong to ask questions. As an Arizona Rh incompatibility birth injury lawyer, Hastings Law Firm focuses exclusively on medical negligence and has the resources to investigate what happened, identify where the standard of care broke down, and hold the responsible parties accountable. Contact us for a free, confidential case evaluation so we can review your records and explain your options.
Understanding Rh Incompatibility and Hemolytic Disease of the Newborn
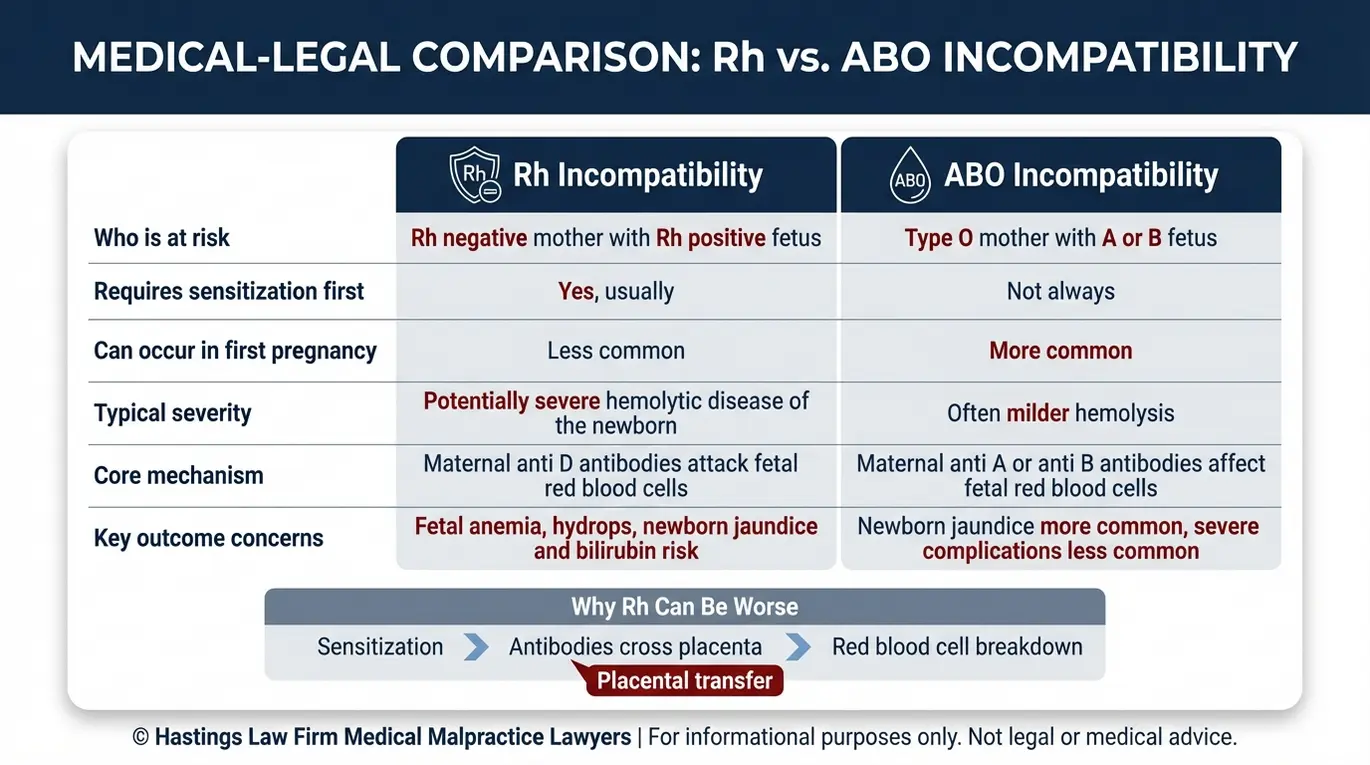
Rh incompatibility occurs when an Rh-negative mother carries an Rh-positive fetus, causing her immune system to produce antibodies that attack the baby’s red blood cells. The Rh factor, a protein known as the D antigen found on the surface of red blood cells, is either present (Rh-positive) or absent (Rh-negative). When a mother lacks this protein and her baby has it, a dangerous immune response can develop.
The process begins with sensitization. During pregnancy or delivery, small amounts of fetal blood can cross the placental barrier and enter the mother’s bloodstream. Her immune system recognizes the Rh-positive cells as foreign and produces antibodies against them. In a first pregnancy, this sensitization event often occurs late enough that the baby is not significantly affected.
But in subsequent pregnancies with an Rh-positive fetus, those antibodies are already present. They cross the placenta, target the baby’s red blood cells, and begin destroying them. This immune attack does not stop on its own; as long as the antibodies are present, they continue to hemolyze, or destroy, fetal cells, worsening the anemia. Research published in PLOS Computational Biology on placental IgG transfer confirms how efficiently maternal antibodies pass through the placenta, especially later in pregnancy.
This destruction of red blood cells leads to hemolytic disease of the newborn (HDN), a condition where the baby becomes severely anemic and develops dangerous levels of bilirubin as the body breaks down the damaged cells. HDN can range from mild jaundice to life-threatening organ failure.
Rh incompatibility is not the only type of blood group conflict. ABO incompatibility also involves a mismatch between maternal and fetal blood types, though it behaves differently. A comparative analysis published in PubMed Central examined treatment outcomes for both conditions, and Rh incompatibility injury attorneys often need to distinguish between the two when building a case.
| Feature | Rh Incompatibility | ABO Incompatibility |
|---|---|---|
| Cause | Rh-negative mother, Rh-positive baby | Mother is type O; baby is type A, B, or AB |
| Sensitization required? | Yes, usually from a prior pregnancy or event | No; can occur in the first pregnancy |
| Typical severity | Can be severe or fatal without treatment | Usually mild to moderate |
| Risk in subsequent pregnancies | Increases significantly with each pregnancy | Does not typically worsen over time |
The Medical Standard of Care for Preventing Rh Sensitization
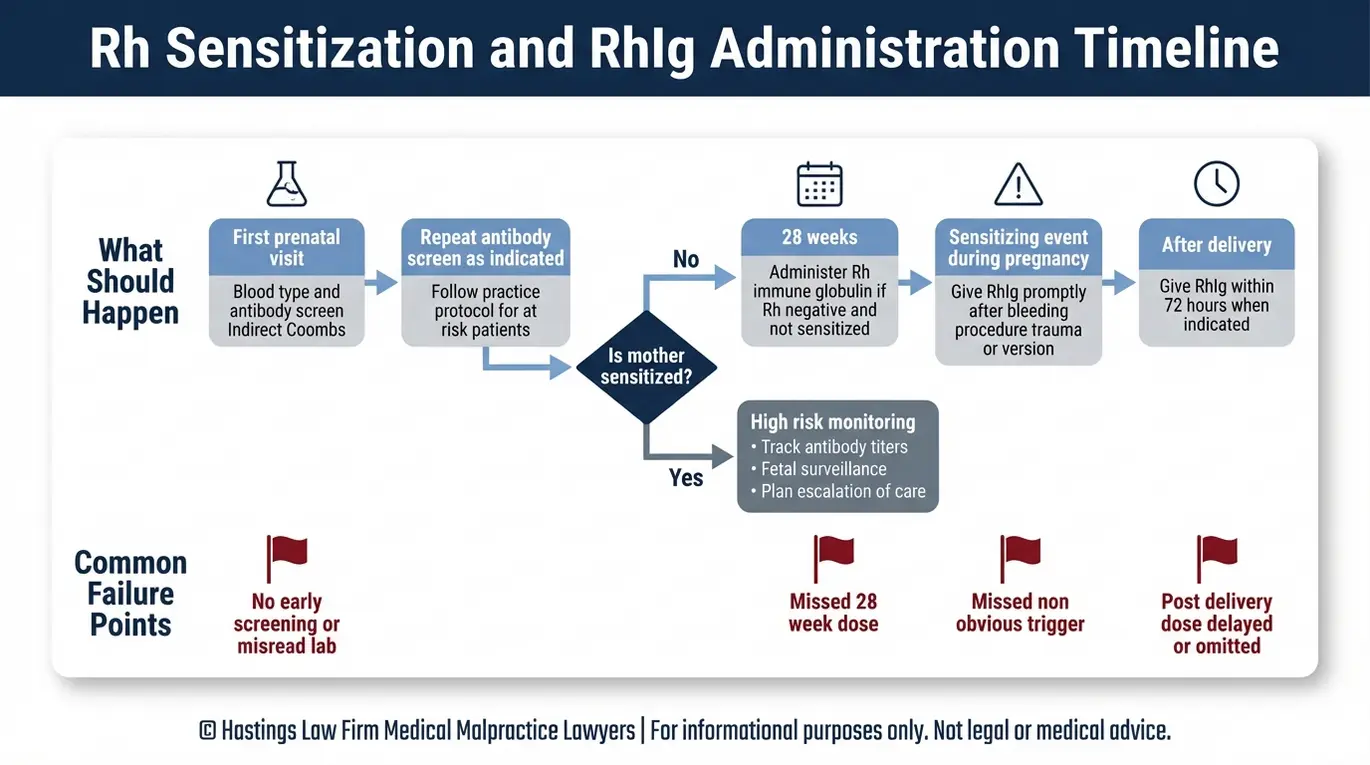
The standard of care mandates that obstetricians screen all pregnant women for blood type and antibodies early in pregnancy and administer Rh immune globulin (RhoGAM) at specific intervals to prevent sensitization. Rh immune globulin (RhoGAM), a blood product that prevents the mother’s immune system from producing anti-Rh antibodies, blocks the recognition of positive cells. When given at the right time, it is remarkably effective.
Screening begins at the first prenatal visit with a comprehensive antibody screening and Indirect Coombs test, a blood test that detects whether the mother has already developed Rh antibodies from a previous pregnancy or sensitizing event. According to the NCBI Bookshelf resource on Rho(D) Immune Globulin, the established protocol calls for RhoGAM administration at 28 weeks of gestation and again within 72 hours after delivery if the baby is confirmed Rh-positive. Missing either of these windows can leave the mother unprotected and allow sensitization to occur.
Our legal team includes former defense attorneys and hospital nurses who previously worked for the systems they now challenge, providing strategic insight into hospital protocols. Failures are not always limited to the 28-week and postpartum doses. The following events also require RhoGAM, and doctors may sometimes overlook them:
- Miscarriage or ectopic pregnancy
- Elective or therapeutic abortion
- Amniocentesis or chorionic villus sampling
- Abdominal trauma during pregnancy
- External cephalic version (manually turning a breech baby)
- Significant vaginal bleeding during pregnancy
Unique Risks of Non-Obvious Sensitization Triggers
Sensitization, the process by which the mother’s immune system begins producing antibodies against Rh-positive blood, does not only happen during delivery. Any event that causes fetal-maternal hemorrhage, meaning fetal blood cells leak into the mother’s circulation, can trigger it. A car accident during pregnancy, a fall, or even a routine procedure like amniocentesis can cause enough mixing of blood to start the immune response.
Many parents are unaware that these events carry Rh-related risk. If a provider fails to recognize the need for RhoGAM after one of these triggers, the sensitization may go undetected until the next pregnancy, when the consequences are far more severe.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Diagnosing and Treating Fetal Anemia and Newborn Complications
Doctors diagnose fetal anemia using Doppler ultrasound to measure blood flow speed and treat severe cases with intrauterine blood transfusions or early delivery followed by phototherapy. The fetal anemia identified by these tests requires careful management to prevent long-term neurological damage. The key diagnostic tool is middle cerebral artery Doppler peak systolic velocity (MCA-PSV), a non-invasive ultrasound measurement that tracks how fast blood flows through the baby’s brain. When a fetus is anemic, its blood becomes thinner and moves faster, producing measurably elevated velocities. A study published in the International Medical Review Press on fetal hydrops and MCA Doppler confirms that MCA-PSV is a reliable, non-invasive predictor of fetal anemia that helps guide the timing of treatment.
When fetal anemia is identified, treatment follows a clear escalation:
- Mild cases: Monitoring with serial Doppler ultrasounds and antibody titer checks.
- Moderate anemia: Intrauterine transfusion (IUT), a procedure where compatible blood is transfused directly into the fetus through the umbilical cord, to correct anemia before delivery.
- Severe or late-stage anemia: Early delivery followed by phototherapy (light therapy that breaks down excess bilirubin in the newborn’s skin) or exchange transfusion for critical hyperbilirubinemia, where dangerously high bilirubin levels require the newborn’s blood to be partially replaced.
The most dangerous outcome of untreated severe fetal anemia is hydrops fetalis, a condition in which massive fluid accumulates in the baby’s tissues and body cavities. Hydrops fetalis carries an extremely high mortality rate. The fluid buildup places immense strain on the fetus’s heart and lungs, often leading to heart failure in utero if not treated aggressively. A Phoenix Rh disease attorney reviewing these cases will look closely at whether providers ordered timely MCA-PSV monitoring and acted on the results.
Proving Medical Malpractice in Rh Incompatibility Cases
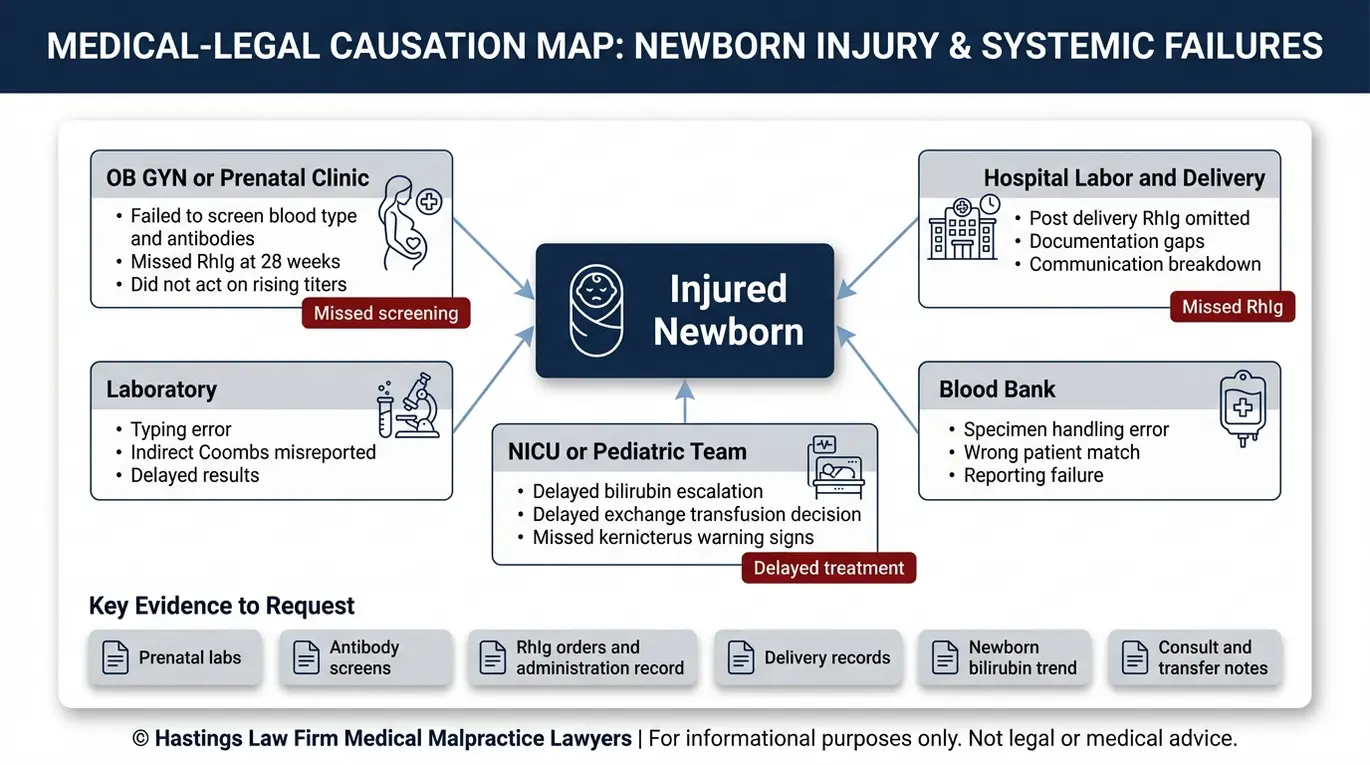
Proving malpractice requires demonstrating that the provider failed to screen for antibodies, neglected to administer RhoGAM, or failed to monitor and treat a sensitized pregnancy, directly causing the infant’s injury. Establishing medical negligence requires a detailed comparison of the actions taken by your providers against the accepted protocols of the obstetrical community. Our legal team uses insider knowledge from former defense attorneys to anticipate how medical facilities might explain these errors.
Failure to screen. If a provider did not check the mother’s blood type and antibody status at the first prenatal visit, any resulting sensitization and fetal harm may trace directly to that omission.
Failure to administer RhoGAM. Missing the 28-week dose, the postpartum dose, or a dose after a sensitizing event like miscarriage or trauma leaves the mother vulnerable. The records should document each administration. Gaps in that documentation can be powerful evidence.
Failure to monitor a sensitized pregnancy. Once antibodies are detected, the standard of care requires regular titer checks and Doppler monitoring. Hyperbilirubinemia, dangerously elevated bilirubin levels in the newborn, can cause kernicterus, a form of permanent brain damage caused by bilirubin deposits in the brain. If rising antibody levels or signs of jaundice were ignored or treated too late, that delay may constitute negligence. Your legal team will scrutinize the fetal monitoring strips and lab reports to pinpoint exactly when the distress became evident.
Multi-party liability. Not every error begins with the obstetrician. According to transfusion-related error data reported to the CDC’s National Healthcare Safety Network Hemovigilance Module, blood typing and crossmatching mistakes do occur. If a laboratory or blood bank misidentified the mother’s Rh type or misreported an Indirect Coombs test result, those entities may share liability. When suing for Rh incompatibility negligence, our team investigates every provider in the chain, including hospital systems, independent labs, and blood banks, to identify where the breakdown occurred.
Our in-house medical staff, including nurse practitioners and board-certified patient advocates, review clinical records alongside our attorneys to reconstruct the timeline of care and identify each point where the standard was not met.
Compensation for Long-Term Injuries and Wrongful Death
Families may recover compensation for past and future medical expenses, life-care planning for permanent disabilities like cerebral palsy, lost earning capacity, and pain and suffering. The financial scope of these cases often extends across a child’s entire lifetime.
A child who develops kernicterus or other brain damage from untreated Rh disease may require ongoing therapies, specialized education, adaptive equipment, and round-the-clock care. Specialized life-care planning, developed by medical and vocational experts, projects these costs over decades. These plans are essential to ensure a settlement or verdict actually covers the child’s real needs rather than a discounted estimate.
In the most tragic cases, severe hydrops fetalis can lead to stillbirth or neonatal death. Families in this situation may pursue a wrongful death claim to recover damages for their loss, including funeral expenses, loss of companionship, and the emotional suffering that follows.
We prepare every case as if it will go to trial from the very beginning. By working with qualified medical experts and building a complete damages picture early, we maintain a firm negotiation posture. Our goal is simple: to ensure any resolution reflects the full, lifetime impact on your child and your family.
Contact the Arizona Birth Injury Attorneys at Hastings Law Firm Today for Help
Rh disease is one of the most preventable complications in modern obstetrics. Our team is led by board-certified trial lawyer Tommy Hastings, who has spent over two decades enforcing accountability and improving patient safety standards. The screenings are routine, and the treatment is effective. When a baby is harmed because a provider skipped a step or missed a critical window, that family deserves answers.
At Hastings Law Firm, our team of attorneys, former defense counsel, and in-house medical professionals investigates these cases with the depth and precision they demand. We understand that your trust in the healthcare system has been shaken, and we are here to help you find the truth about what happened.
If your child was injured by what you believe was a failure to prevent or manage Rh incompatibility, contact our Arizona medical malpractice firm for a free, confidential case evaluation. You pay no fees or costs unless we recover compensation on your behalf. Call us today or complete our online form to take the first step.
Frequently Asked Questions About Rh Incompatibility Birth Injury in Arizona

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
