

Arizona Retinopathy of Prematurity Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Retinopathy of Prematurity is a potentially blinding eye disorder that affects some premature infants and can progress silently without careful NICU monitoring. The condition involves abnormal retinal blood vessel growth that can lead to scarring, retinal detachment, and permanent vision loss. The most important issue is whether accepted screening, oxygen management, and timely treatment were followed, since missed exams or delayed intervention can allow preventable harm to become irreversible. If you or a loved one were harmed or worse due to Retinopathy of Prematurity malpractice in Arizona, contact Hastings Law Firm for a free, confidential case review.

Top Rated Arizona Medical Attorneys for Infant Blindness Claims
What You Should Know About Premature Infant Blindness Claims in Arizona:
- Permanent blindness can result when Retinopathy of Prematurity progresses to retinal detachment and the damage is not caught in time.
- Preventable vision loss can occur when required eye screening is delayed or missed for at risk premature infants.
- Irreversible harm can follow when NICU oxygen levels are mismanaged and abnormal retinal vessel growth accelerates.
- Options for effective treatment can narrow when urgency markers such as Plus disease are not recognized or acted on promptly.
- Long term financial impact can be substantial because compensation is described as covering medical care, life care needs, and loss of earning capacity.
- Responsibility can extend beyond one clinician when neonatologists, ophthalmologists, and hospitals share duties for screening, communication, and protocol enforcement.
- Recovery can be limited if time related legal rules are missed because Arizona medical malpractice deadlines and tolling for minors are discussed.
- Disputes about what happened can turn on documentation because exam findings, referrals, and NICU records are expected to be clearly recorded and communicated.

A Healthcare Focused Law Firm
When a premature baby loses their sight to a condition that could have been caught and treated, families deserve honest answers about what went wrong. Retinopathy of Prematurity, or ROP, is one of the leading causes of infant blindness, and in many cases, the damage is preventable with proper screening and timely intervention.
If your child was born prematurely and now faces vision loss or blindness, you may be wondering whether the medical team responsible for your baby’s care met the accepted standard. As an Arizona Retinopathy of Prematurity lawyer, Hastings Law Firm focuses exclusively on medical malpractice, and our team includes in-house medical professionals who understand exactly what NICU records should show. We welcome you to contact us for a free, confidential case evaluation so we can review what happened and help you understand your options.
Understanding Retinopathy of Prematurity and Preventable Vision Loss
Retinopathy of Prematurity (ROP) is a potentially blinding eye disorder affecting premature infants weighing about 3.3 pounds (1,500 grams) or less where abnormal blood vessels grow in the retina and can lead to detachment. In a full-term pregnancy, retinal blood vessels finish developing shortly before birth. But in premature infants, that process is incomplete. After delivery, abnormal blood vessel growth can occur in an irregular pattern, spreading into areas where the vessels do not belong.
These fragile vessels may leak or bleed, creating scar tissue that pulls on the retina. If the scarring becomes severe, it can cause retinal detachment, a condition where the retina separates from the back of the eye, resulting in permanent vision loss or total blindness. Because the retina does not have pain fibers, this damage occurs silently, making vigilant monitoring by NICU staff absolutely critical.
Not every case of ROP results from medical error. Some degree of abnormal vessel growth can occur even with proper care. The distinction that matters, and what ROP attorneys in Arizona evaluate closely, is whether the medical team followed accepted protocols for monitoring and treatment.
When screening is delayed, oxygen levels are mismanaged, or treatment windows are missed, a preventable complication becomes preventable negligence. While nature dictates the prematurity, the medical team dictates the safety of the environment in which the infant develops.
Common Causes of ROP and NICU Malpractice
NICU malpractice contributes to ROP when medical staff fail to properly manage oxygen levels or neglect mandatory screening protocols for at-risk infants. Understanding the risk factors and how negligence occurs is essential for families trying to make sense of their child’s diagnosis.
Two primary biological risk factors make certain newborns more vulnerable to ROP:
- Low gestational age: Infants born before 30 weeks of gestation, meaning the number of weeks the pregnancy has progressed, have significantly underdeveloped retinal blood vessels.
- Low birth weight: Babies weighing less than 1,500 grams (about 3.3 pounds) are at elevated risk. This is because their bodies and eyes are not yet mature enough to regulate normal vascular growth.
Oxygen therapy is one of the most carefully studied contributors to ROP. Premature infants often need supplemental oxygen to survive, but improper management of oxygen saturation levels, the practice of keeping blood oxygen within a precise range, can accelerate abnormal vessel growth. When oxygen is too high, vessel growth stops; when it is removed, the vessels can grow back aggressively and in a disorganized manner. Research published by the National Institutes of Health on oxygen saturation outcomes in preterm infants has documented how both excessively high and dangerously low oxygen levels contribute to ROP development.
Beyond oxygen management, NICU teams are responsible for tracking clinical indicators that may worsen ROP risk. Failure to monitor anemia, poor weight gain, or unstable respiratory status can allow the condition to progress undetected. An Arizona ROP lawyer examines these records carefully to determine whether the NICU team’s care met the standard expected of reasonably competent medical professionals.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Mandatory Screening Guidelines and Failure to Monitor
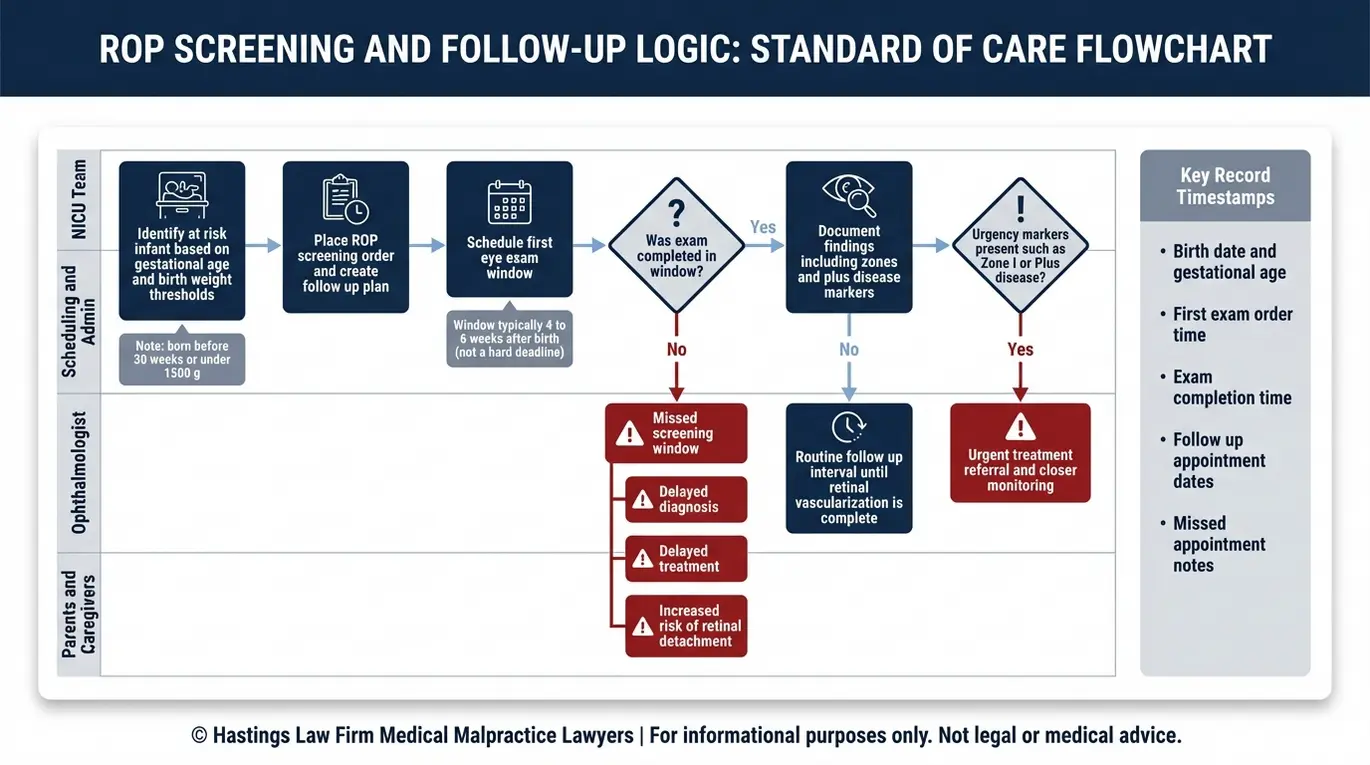
Standard of care dictates that all infants born before 30 weeks or weighing less than 1500 grams must undergo precise ophthalmologic screening examinations at specific intervals. These are not optional recommendations. They are established medical guidelines that NICUs are expected to follow.
An ROP screening examination, a dilated eye exam performed by an ophthalmologist with pediatric retinal expertise, allows doctors to assess the development of blood vessels in the infant’s retina. The initial screening typically occurs four to six weeks after birth, and the timing depends on the infant’s gestational age at delivery.
What families should know about standard of care protocols for screening:
- The first eye exam should occur no later than four to six weeks after birth for eligible infants. This window is critical because ROP can progress to advanced stages very quickly during early development.
- Follow-up exams must continue at regular intervals until retinal vascularization, the complete growth of normal blood vessels, is finished. These appointments ensure that any late-onset vessel changes are identified before they cause permanent damage.
- A single missed or delayed exam can allow the disease to progress beyond the point where treatment is effective. Medical staff must maintain a strict schedule to protect the infant’s long-term sight.
- The examining doctor must document findings clearly so the NICU team can act on any changes, such as the sudden appearance of aggressive vascular twisting. Clear communication between the eye specialist and the neonatal team is the primary defense against diagnostic errors.
Missing even one screening window can be the difference between treatable ROP and irreversible blindness. A Retinopathy of Prematurity lawyer in Arizona investigates whether every required exam was ordered, performed on time, and properly documented.
Clinical Urgency Markers and Disease Progression
ROP is classified by location and severity using a zone and stage system. Clinical markers are visual signs that indicate how quickly the disease is moving. ROP zones, which describe where the disease appears on the retina, help clinicians determine the immediate threat level: Zone I is the most central and dangerous area, Zone II is the middle ring, and Zone III is the outermost region. Disease found in Zone I demands the most urgent response because it threatens the area of sharpest vision.
Equally important is the presence of Plus disease, a condition marked by abnormal dilation and twisting of retinal blood vessels. Plus disease signals that the ROP is aggressive and progressing rapidly. When an examiner identifies Plus disease, particularly in Zone I or Zone II, it typically triggers an immediate referral for treatment. A failure to recognize or act on these urgency markers can result in irreversible damage within days.
Medical Interventions and Surgical Errors in ROP Care
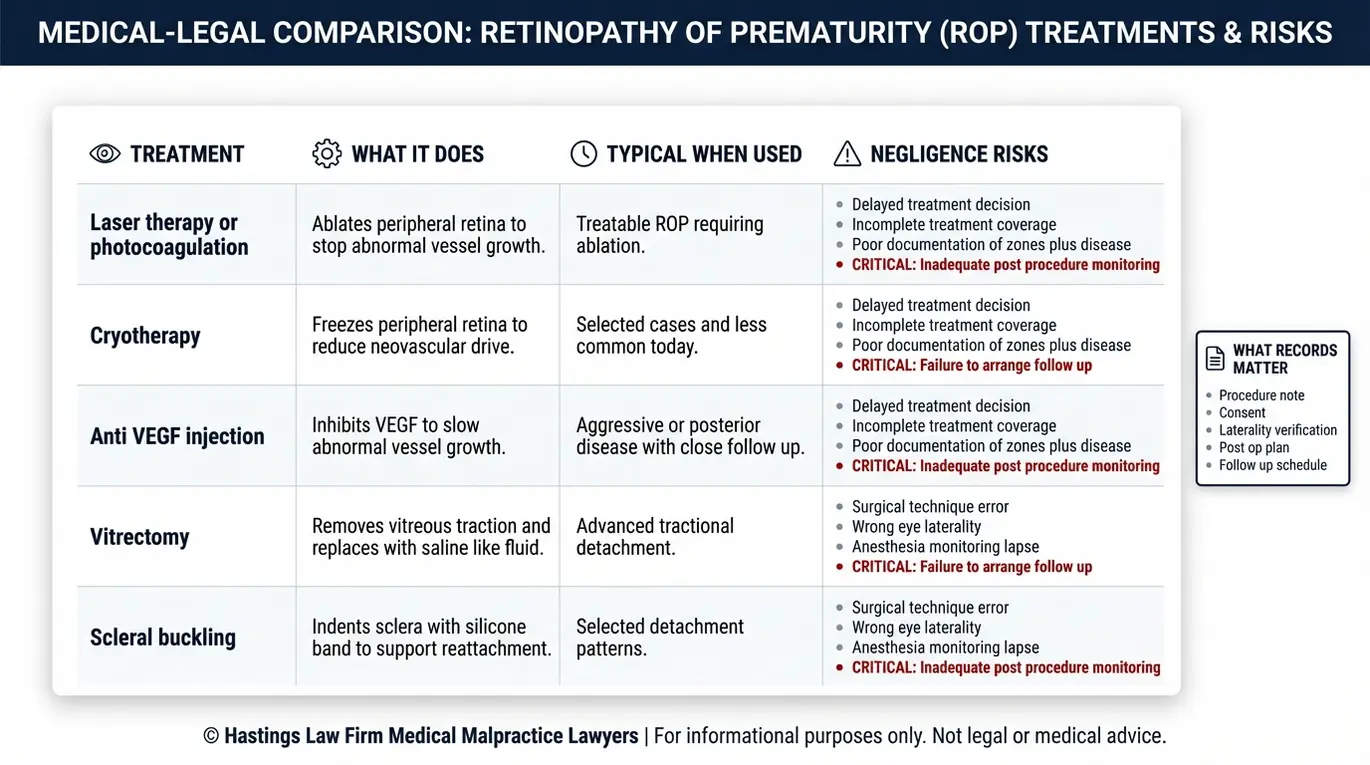
Timely treatment for ROP includes laser therapy or cryotherapy to stop abnormal vessel growth, while advanced stages may require vitrectomy or scleral buckling surgeries. When treatment is delayed or performed incorrectly, the consequences for the infant can be devastating.
Laser photocoagulation, a procedure that uses a focused laser beam to burn and seal off abnormal blood vessels in the peripheral retina, remains the gold standard for treating ROP before it reaches advanced stages. Cryotherapy, which freezes portions of the retina to achieve a similar effect, is less commonly used today but may still be applied in certain clinical scenarios. Research comparing treatment modalities, including studies published in the National Library of Medicine on anti-VEGF therapy versus laser therapy outcomes, continues to refine best practices for intervention.
| Treatment Type | Procedure Description | Potential Negligence Risks |
|---|---|---|
| Laser Photocoagulation | Laser seals abnormal blood vessels in the peripheral retina | Delayed referral, incomplete treatment coverage, failure to schedule timely follow-up |
| Cryotherapy | Freezing probe applied to the outer retina to halt vessel growth | Use when laser is more appropriate, inadequate application |
| Anti-VEGF Injections | Medication injected into the eye to inhibit abnormal vessel growth | Insufficient long-term monitoring after injection, missed reactivation |
| Vitrectomy | Surgical removal of vitreous gel and scar tissue, replaced with saline solution | Delayed surgery allowing full retinal detachment, surgical error during the procedure |
| Scleral Buckling | A silicone band placed around the eye to push the wall of the eye inward, supporting retinal reattachment | Failure to recommend surgery when indicated, improper band placement |
Detailed Surgical Mechanics
When ROP advances to stage 4 or 5, surgical intervention becomes necessary to prevent total blindness. Surgical mechanics are the physical techniques used to repair structural damage in the eye. A vitrectomy, a surgical procedure that involves removing the vitreous gel from inside the eye along with any scar tissue pulling on the retina, uses saline solution to allow the retina to settle back into position. Scleral buckling, an approach utilizing a silicone band placed around the exterior of the eye to gently indent the eye wall inward, helps relieve traction on the retina and supports reattachment.
Both procedures carry significant risks, and the decision to operate must be made with careful attention to timing and the infant’s overall condition. Arizona Retinopathy of Prematurity attorneys evaluate whether surgical decisions were made appropriately and whether any delays allowed the disease to progress beyond the point of effective repair.
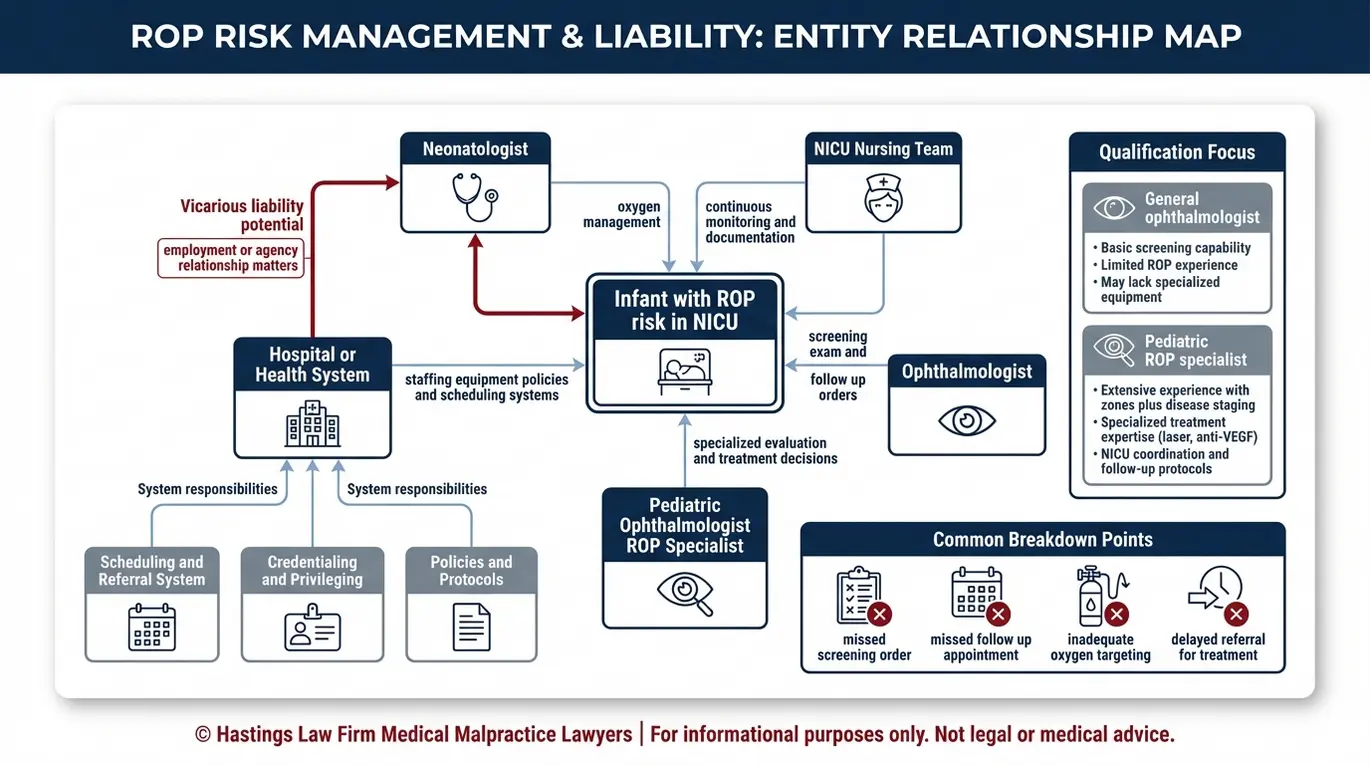
Identifying Liability and Responsible Medical Providers
Liability for ROP blindness often extends to neonatologists who manage NICU care, ophthalmologists responsible for screenings, and the hospital for systemic failures.
The NICU team and the eye specialist share overlapping duties when it comes to ROP prevention. Neonatologists, who are doctors specializing in the care of newborn infants, are responsible for oxygen management and ensuring timely referrals for eye exams. The ophthalmologist or pediatric ophthalmologist must perform exams on schedule and communicate findings that require urgent action. When communication breaks down between these providers, infants fall through the cracks.
Hospitals can also bear medical liability for failing to maintain adequate staffing, lacking proper screening equipment, or not enforcing protocols that ensure at-risk infants are examined on time. One factor we look at closely is whether the examining physician was a qualified pediatric ROP specialist or a general ophthalmologist without specific training in neonatal retinal disease. Families can verify a physician’s credentials through resources like Certification Matters. An ROP malpractice lawyer in Arizona works to identify every responsible party and determine how the system failed.
Recovering Damages for Lifelong Vision Loss
Compensation in ROP cases covers past medical bills, future life care costs, pain and suffering, and loss of earning capacity for the blinded child. Because ROP-related blindness is permanent, the financial impact stretches across the child’s entire lifetime. To ensure a settlement covers these decades of need, an Arizona ROP attorney works with life-care planners to project costs over 50 to 70 years, accounting for medical inflation and necessary technology upgrades.
We pursue both economic and non-economic damages:
- Past and future medical expenses: Surgeries, specialist visits, ongoing eye care, and any corrective procedures. This includes specialized care from pediatric ophthalmologists throughout childhood and adulthood.
- Assistive technology and home modifications: Screen readers, braille displays, adaptive equipment, and accessibility renovations which can cost thousands of dollars over a lifetime.
- Specialized education: Individualized Education Programs (IEPs), orientation and mobility training, and braille instruction.
- Mobility aids and support: Guide dogs, mobility canes, and long-term training programs which require regular retraining and replacement.
- Loss of earning capacity: The income the child will likely never be able to earn due to permanent disability.
- Pain, suffering, and loss of enjoyment of life: The profound impact of growing up without sight.
The CDC’s Vision and Eye Health data documents the significant economic burden associated with vision loss, reinforcing why these cases require careful life-care planning.
Practical Long-Term Support Needs
A lawyer for premature infant blindness must account for needs that extend well beyond medical bills. Long-term support refers to the non-medical services a child needs to manage the world without sight. Children with ROP-related blindness require individualized education programs tailored to their visual impairment, professional mobility training to learn safe independent travel, and eventually assistive technology for education and employment. Many families also face costs for guide dog training and ongoing orientation services. Every element of the child’s future must be projected and documented to ensure the settlement or verdict reflects the true cost of the injury.
Why Choose Hastings Law Firm for Your Arizona ROP Case
Hastings Law Firm offers a trial-ready approach with board-certified leadership and in-house medical staff, ensuring families of blinded infants receive a firm, trial-ready posture against powerful hospital systems. Our founder, Tommy Hastings, is Board Certified in Personal Injury Trial Law by the Texas Board of Legal Specialization, a distinction held by fewer than 2% of Texas attorneys. That level of specialization matters in cases involving complex neonatal medicine.
We are not a high-volume settlement firm. Every case is prepared from day one as if it will go before a jury. Our in-house medical staff, including nurse practitioners and Board Certified Patient Advocates, review NICU records, oxygen logs, and screening documentation to identify exactly where the standard of care was breached. Former defense attorneys on our team know how hospitals and their insurers will try to deflect responsibility, and we build our cases to address those arguments head-on.
Our Phoenix office gives Arizona families direct access to our team. And because we handle these cases on a contingency fee basis, you can hire an experienced Arizona Retinopathy of Prematurity Lawyer with no upfront fees or costs unless we recover compensation on your behalf.
Contact the Arizona Birth Injury Attorneys at Hastings Law Firm Today for Help
Your child’s blindness may have been preventable, and you deserve to know what happened. At Hastings Law Firm, we are committed to helping families uncover the truth and hold negligent medical providers accountable so that what happened to your child does not happen to another family.
Our confidential consultation is led by a patient advocate who will listen to your story and help determine whether your child’s care fell below the accepted standard. Time matters in these cases, as evidence can be lost and legal deadlines do apply, so we encourage you to reach out as soon as you are ready.
If you are looking for an Arizona Retinopathy of Prematurity lawyer who will treat your family with the respect and dedication your child deserves, contact Hastings Law Firm today. There is no fee unless we win.
Frequently Asked Questions About Retinopathy of Prematurity in Arizona

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
