

Arizona Polyhydramnios Mismanagement Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: May 6, 2026
Polyhydramnios involves excess amniotic fluid that can strain the uterus and raise the risk of dangerous labor complications when it is not recognized and managed appropriately. The condition is typically monitored with ultrasound measurements, and missed warning signs or delayed responses can contribute to oxygen deprivation and lasting newborn harm. Treatment choices also matter because some interventions carry their own risks when used without careful oversight. If you or a loved one were harmed or worse due to polyhydramnios mismanagement in Arizona, contact Hastings Law Firm for a free, confidential case review.
Top Rated Arizona Birth Injury Attorneys for Polyhydramnios Cases
What You Should Know About Excessive Amniotic Fluid Birth Injury Claims in Arizona:
- Lasting newborn harm can occur when uncontrolled polyhydramnios leads to oxygen deprivation during emergencies such as umbilical cord prolapse or placental abruption.
- Options for safer outcomes can narrow quickly when elevated fluid levels are not acted on with appropriate urgency.
- Serious complications can follow when providers document abnormal ultrasound findings but do not investigate the underlying cause.
- Disputes about whether care was appropriate often turn on whether ultrasound measurements were accurately taken, correctly interpreted, and repeated when needed.
- Preventable injury risk can increase when key contributing factors are not identified, such as gestational diabetes or fetal anomalies.
- Additional harm can result when amnioreduction is performed negligently, since the procedure carries risks such as infection or premature rupture of membranes.
- Cardiac complications can occur when indomethacin is used without careful limits and monitoring, including the risk of premature closure of the fetal ductus arteriosus.
- Recovery for long term disabilities can be shaped by the projected cost of lifelong care, including therapy needs and adaptive equipment.
- Case outcomes can depend on whether medical records show timely recognition of escalating risk, including fetal monitoring data and ultrasound reports.
- Accountability can hinge on whether electronic records reveal when test results were reviewed and whether critical information was ignored.

A Healthcare Focused Law Firm
When your pregnancy was supposed to be closely monitored and something still went wrong, the confusion and grief can feel overwhelming. If your child suffered a birth injury that you believe was connected to high amniotic fluid levels that were not properly managed, you deserve honest answers about what happened and why.
At Hastings Law Firm, our legal and medical team focuses exclusively on medical malpractice cases, including those involving polyhydramnios mismanagement during pregnancy. As an Arizona polyhydramnios mismanagement lawyer team with in-house nurse consultants and a national network of obstetric experts, we examine the medical records, identify where the standard of care may have been violated, and build the case from there. If you have questions about your family’s situation, we offer a free, confidential case evaluation with no fee unless we recover compensation on your behalf.
Understanding Polyhydramnios and the Legal Standard of Care
Polyhydramnios is a condition defined by an excessive accumulation of amniotic fluid during pregnancy, affecting roughly 1% of pregnancies and requiring careful monitoring to prevent serious complications. Also referred to as hydramnios, the condition means that the fluid surrounding the baby in the uterus has exceeded normal levels. That excess amniotic fluid can place significant strain on the uterus and increase the risk of dangerous delivery complications.
According to the NCBI Bookshelf overview of polyhydramnios, the condition ranges from mild to severe and can develop gradually or rapidly. When fluid levels rise, the uterus stretches beyond its normal capacity, a situation known as uterine overdistension, which is the abnormal stretching of the uterine wall caused by excessive internal volume. This overdistension can trigger preterm contractions, make it harder for the baby to settle into a head-down position, and set the stage for emergencies during labor.
The legal standard of care, meaning the accepted level of treatment that a reasonably competent obstetrician would provide under similar circumstances, requires doctors to monitor amniotic fluid levels through regular ultrasound assessments. When a provider identifies elevated fluid, the standard typically calls for investigating the underlying cause and adjusting the care plan accordingly.
Two primary ultrasound measurements are used to assess fluid volume. The Amniotic Fluid Index (AFI), which calculates the sum of the deepest vertical pocket in each of four uterine quadrants, is the more commonly used method. The Single Deepest Pocket (SDP), a measurement of only the single largest vertical pocket of fluid visible on the scan, provides an alternative metric.
While AFI is more commonly used, it can sometimes overestimate fluid volume, leading to unnecessary interventions. Conversely, SDP is considered by many experts to be a more specific metric, reducing the likelihood of a false-positive diagnosis while still identifying genuine risks. Understanding these distinctions is critical when reviewing medical records for potential malpractice.
Diagnostic Comparison of AFI vs Single Deepest Pocket
Doctors use two methods to measure amniotic fluid on ultrasound. These diagnostic tools help physicians determine if fluid levels have become unsafe.
| Measurement Method | How It Works | Polyhydramnios Threshold | Clinical Significance |
|---|---|---|---|
| Amniotic Fluid Index (AFI) | Sum of the deepest vertical pocket in each of four uterine quadrants | Greater than 24–25 cm | More commonly used; can overestimate fluid in some cases |
| Single Deepest Pocket (SDP) | Measurement of the single largest vertical pocket of fluid | Greater than 8 cm | May be more specific; increasingly favored in research settings |
Both methods depend on accurate technique and correct interpretation. If a provider misreads an AFI of 26 cm as normal, or fails to repeat an SDP measurement when initial readings are borderline, the delay in diagnosis can constitute a breach of the standard of care. An Arizona polyhydramnios mismanagement lawyer evaluates whether these measurements were properly taken, correctly interpreted, and acted upon in a timely manner.

Recognizing Risk Factors and Missed Warning Signs
Obstetricians are required to screen for risk factors that commonly underlie polyhydramnios, including gestational diabetes and fetal anomalies. When a provider fails to identify these contributing conditions, it may constitute medical negligence because treating polyhydramnios effectively depends on understanding its cause.
Gestational diabetes is one of the most well-documented drivers of elevated amniotic fluid. High maternal blood sugar levels cause the baby to produce more urine, which directly increases the volume of fluid in the uterus. Research published by PubMed Central on polyhydramnios at term in gestational diabetes reinforces the clinical connection between poorly controlled glucose levels and excess amniotic fluid. When a doctor fails to screen for or adequately manage gestational diabetes, the resulting fluid buildup can go unaddressed until complications develop.
Fetal anomalies, meaning structural or functional abnormalities in the developing baby, are another leading cause. Certain congenital abnormalities can affect the baby’s ability to swallow amniotic fluid, which is one of the body’s natural mechanisms for regulating fluid volume. If the baby cannot swallow normally due to a gastrointestinal obstruction or neurological condition, fluid accumulates. Identifying these anomalies early through targeted ultrasound is part of the expected diagnostic workup.
The baby’s size and position also matter. Macrosomia, a condition where the baby grows significantly larger than average, often correlates with excess fluid and gestational diabetes. Fetal malposition, particularly breech presentation, can both result from and be worsened by polyhydramnios because the excess fluid gives the baby more room to shift out of position. Identifying these anomalies early through targeted ultrasound is part of the expected diagnostic workup.
A responsible provider does more than simply document high fluid levels on an ultrasound report. The standard of care calls for investigating why the fluid is elevated. Medical providers cannot simply note an abnormality and move on; the standard of care dictates a proactive approach.
If a mother presents with rapid abdominal growth or shortness of breath, symptoms often associated with severe polyhydramnios, the physician must rule out conditions like gestational diabetes immediately. Ignoring these clinical signs deprives the mother and baby of essential management strategies that could mitigate harm. Key risk factors that doctors should screen for include:
- Gestational diabetes (glucose tolerance testing)
- Fetal swallowing abnormalities detected on ultrasound
- Congenital abnormalities affecting the gastrointestinal tract or nervous system
- Macrosomia or accelerated fetal growth
- Fetal malposition, including breech presentation
- Rh factor incompatibility or other causes of fetal anemia
- Multiple gestation (twins or higher-order pregnancies)
An Arizona polyhydramnios mismanagement lawyer and the medical professionals supporting the legal team review whether these screenings were ordered, whether results were followed up on, and whether the care plan reflected the findings. A failure to diagnose polyhydramnios or investigate its underlying cause can delay treatment that might have prevented a birth injury.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

The Dangers of Inaction and Preventable Birth Injuries
Uncontrolled polyhydramnios creates serious obstetric risks, including umbilical cord prolapse, placental abruption, and preterm labor, each of which can lead to severe oxygen deprivation and permanent brain damage in the newborn. When uncontrolled polyhydramnios is identified but not properly managed, the window for safe intervention can close rapidly.
Umbilical Cord Prolapse
Umbilical cord prolapse occurs when the umbilical cord slips through the cervix ahead of the baby, often carried by the sudden rush of fluid when the membranes rupture. A prolapsed cord occurs when it precedes the baby into the birth canal, potentially cutting off oxygen delivery. In polyhydramnios cases, the sheer volume of excess amniotic fluid increases this risk dramatically. When the waters break, the high volume of fluid creates a powerful wash that can sweep the cord out.
Obstetricians must be prepared for this possibility during delivery, often by having an operating room on standby if manual elevation of the fetal head is required to relieve pressure on the cord while preparing for a C-section. Once the cord is compressed, blood flow and oxygen delivery to the baby can be cut off within minutes. This is a time-critical emergency that demands immediate delivery.
Placental Abruption
Placental abruption is the premature separation of the placenta from the uterine wall before delivery. This condition interrupts the essential exchange of oxygen and nutrients through the placental attachment. In polyhydramnios, this can happen during rapid decompression, such as when membranes rupture suddenly and the uterus contracts sharply around a reduced volume. Abruption also puts the mother at risk of postpartum hemorrhage and other life-threatening complications.
Preterm Labor and Premature Birth
The overdistension caused by excessive fluid can trigger uterine contractions well before the pregnancy reaches full term. Early delivery often requires specialized care in a neonatal unit. Doctors must carefully balance the risk of early delivery against the risks of continuing a pregnancy with severe fluid overload. If delivery is expedited, the baby may require admission to the NICU for respiratory support. Premature birth carries its own cascade of risks, including underdeveloped lungs, difficulty regulating body temperature, and a higher likelihood of requiring extended care in the NICU.
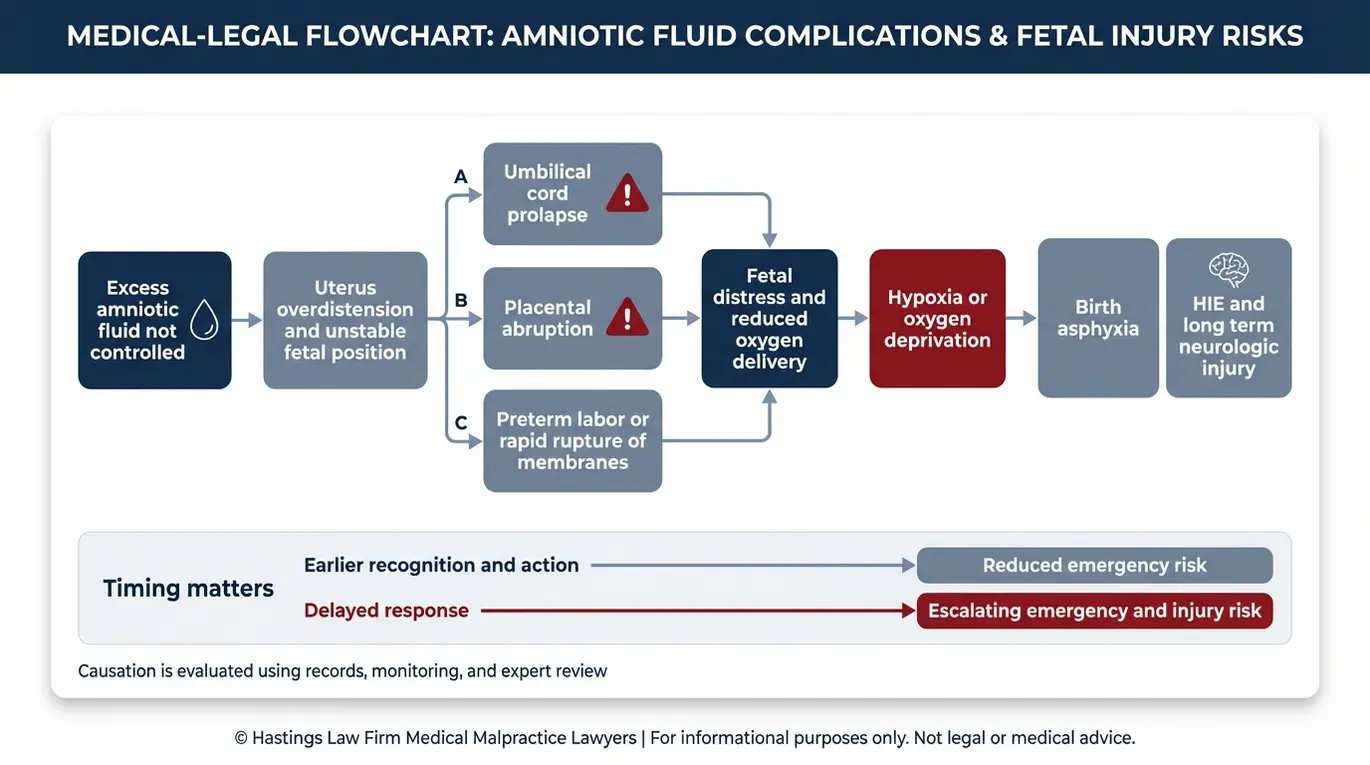
The Path from Complication to Brain Injury
Research published in PLOS ONE on polyhydramnios management and outcomes documents the elevated rates of adverse outcomes associated with poorly managed cases. The chain from untreated polyhydramnios to lasting harm often follows a recognizable pattern:
- Excess amniotic fluid goes unmanaged or undertreated
- An acute event occurs (cord prolapse, abruption, or precipitous preterm labor)
- The baby experiences fetal distress and hypoxia, a dangerous reduction in oxygen reaching the brain
- Prolonged oxygen deprivation leads to birth asphyxia
- The resulting brain damage may be diagnosed as Hypoxic-Ischemic Encephalopathy (HIE), a specific type of brain injury caused by inadequate oxygen and blood flow
- Long-term consequences can include cerebral palsy, seizure disorders, and developmental delays
The severity of the injury often depends on the duration of the hypoxic event. Every minute of delay in restoring oxygen significantly increases the likelihood of permanent cortical damage. An Arizona polyhydramnios mismanagement lawyer examines the medical timeline to determine whether providers recognized these escalating risks and responded appropriately, or whether inaction allowed a preventable injury to occur.
Failure to Treat and Improper Medical Interventions
The standard of care may require active interventions such as therapeutic amnioreduction or medication to reduce dangerously high fluid levels, and a failure to implement these treatments in a timely manner can form the basis of a malpractice claim.
Expectant Management vs. Active Intervention
Not every case of polyhydramnios demands immediate procedural intervention. In mild cases, expectant management, which involves close monitoring with serial ultrasounds and fetal assessments, may be appropriate. This approach requires vigilance, ensuring that any sudden change in fetal movement or maternal symptoms triggers an immediate re-evaluation. If delivery is expedited, the baby may require admission to the NICU for respiratory support. But when fluid levels are severe or symptoms are progressing, continuing to “watch and wait” without escalating care can fall below the accepted standard.
Amnioreduction
Amnioreduction, also called therapeutic amniocentesis, is a procedure where a needle is inserted into the uterus to drain excess amniotic fluid. It can relieve uterine overdistension, reduce the risk of preterm labor, and improve the baby’s positioning.
However, the procedure itself carries risks, including infection, premature rupture of membranes, and placental abruption. Repeated procedures may be necessary if fluid re-accumulates rapidly, each time exposing the pregnancy to potential infection or membrane rupture.
The technical skill of the physician performing the reduction is important to safety. When amnioreduction is performed negligently, the treatment itself can cause harm.
Indomethacin and Medication-Related Risks
Indomethacin, a medication sometimes prescribed to reduce fetal urine output and slow the accumulation of amniotic fluid, can be effective but carries a well-documented risk: premature closure of the fetal ductus arteriosus, a blood vessel in the baby’s heart that must remain open during pregnancy. Providers must carefully weigh these medication-specific risks against potential benefits.
According to research published in PubMed Central on indomethacin-induced ductus arteriosus closure, this complication can occur even at standard doses, particularly when the medication is used after 32 weeks of gestation. Strict adherence to dosage guidelines and gestational age limits is non-negotiable to prevent cardiac complications.
Providers prescribing indomethacin are expected to monitor the baby’s heart with regular echocardiograms and limit the duration of treatment. Key risks and monitoring failures we look for in these cases include:
- Prescribing indomethacin beyond 32 weeks without documented clinical justification
- Failing to order serial fetal echocardiograms to monitor the ductus arteriosus
- Continuing the medication after signs of ductal constriction appear
- Not discussing the risks of the drug with the patient (informed consent failures)
- Choosing indomethacin when safer alternatives or amnioreduction may have been more appropriate
An Arizona polyhydramnios mismanagement lawyer works alongside medical experts to evaluate whether the treatment decisions made in your case met the standard of care.

Proving Malpractice in Arizona Polyhydramnios Cases
To prevail in a malpractice claim in Arizona, the injured party must prove that the healthcare provider owed a duty of care, breached that duty through negligent management of amniotic fluid levels, and that the breach directly caused the child’s injury. Arizona law establishes a clear framework for these claims, and meeting each element requires strong medical evidence and qualified expert support.
Arizona common law requires proof of four elements in medical malpractice cases:
- Duty of Care: The provider had a doctor-patient relationship and was responsible for managing the pregnancy.
- Breach of Duty: The provider failed to meet the accepted standard of care, such as missing an abnormal AFI reading, failing to screen for gestational diabetes, or delaying necessary treatment for polyhydramnios. Establishing medical negligence involves demonstrating that the actions taken fell below accepted standards.
- Causation: The breach directly caused or materially contributed to the infant’s injury. Defense attorneys frequently attempt to attribute the injury to genetic factors or pre-existing conditions. Overcoming these defenses requires a meticulous analysis of the pathology reports and placental, cord, and blood gas data to draw a direct line between the fluid mismanagement and the brain injury.
- Damages: The child suffered measurable harm, whether physical, neurological, or developmental, that resulted in medical expenses, ongoing care needs, or other losses.
Arizona Revised Statutes § 12-563 codifies the standards for proving breach and causation, requiring that the provider failed to exercise the degree of care expected of a reasonably prudent healthcare provider and that this failure proximately caused the injury.
Expert testimony is essential in establishing the breach. Arizona requires that a qualified medical professional, typically a board-certified obstetrician or maternal-fetal medicine specialist, review the case and testify about what the standard of care required and how the provider fell short. These experts rely on their clinical experience to explain complex obstetric concepts to a jury. They differentiate between an unavoidable complication and one resulting from provider error, clarifying whether a reasonably prudent doctor would have acted differently.
Our team gathers and analyzes the specific evidence needed to build each element. This includes fetal heart monitor strips, serial ultrasound reports, nursing notes, and delivery records. Electronic medical records often contain an audit trail, revealing exactly when a doctor reviewed a test result or entered an order.
This digital footprint can be important in proving that a provider ignored critical information or failed to respond with appropriate urgency. Our firm, led by board-certified trial lawyer Tommy Hastings, uses a structured process to reconstruct the clinical timeline minute by minute to identify where decisions were made, where they were delayed, and where the standard of care was not met. As an Arizona polyhydramnios mismanagement lawyer team that includes former defense attorneys and in-house nurse consultants, we understand how hospitals document care and how defense teams frame their arguments.
Calculating Damages for Long-Term Disabilities
Families of children injured by polyhydramnios mismanagement may be entitled to compensation for past and future medical expenses, life care planning costs, pain and suffering, and lost earning capacity. When a birth injury results in a condition like cerebral palsy or Hypoxic-Ischemic Encephalopathy, the financial impact extends across the child’s entire lifetime.
The cost of raising a child with a serious neurological injury is substantial. Ongoing physical therapy, occupational therapy, and adaptive equipment can amount to millions of dollars over a lifetime. Compensation must be sufficient to address developmental delays and motor function deficits that emerge as the child grows.
A detailed life care plan, developed with medical and vocational experts, is an important tool in quantifying these needs. Medical and Life Care Consulting Services’ overview of pediatric life care planning outlines best practices for supporting children with disabilities through structured, evidence-based planning. This thorough document projects costs decades into the future, accounting for inflation and the changing needs of the child as they transition from adolescence to adulthood.
Economic damages in these cases typically include past and future medical costs, rehabilitation expenses, assistive technology, and the child’s diminished ability to earn income as an adult. Non-economic damages address the less tangible but equally real losses: physical pain, emotional suffering, loss of enjoyment of life, and the impact on the family as a whole. No amount of money can undo the trauma of a birth injury, but these damages acknowledge the profound shift in the family’s reality and the child’s loss of a carefree childhood.
Our goal as an Arizona polyhydramnios mismanagement lawyer team is to secure the financial resources your child needs for a lifetime of care, not just for today’s bills. We work with economists, life care planners, and medical specialists to present a complete and accurate picture of what your family will need going forward.
Contact the Arizona Birth Injury Attorneys at Hastings Law Firm Today for Help
You do not have to face the aftermath of a preventable birth injury alone. If your child was harmed by what you believe was the mismanagement of polyhydramnios, our team is ready to listen, review your medical records, and give you an honest assessment of your legal rights.
Hastings Law Firm handles these cases on a contingency fee basis, meaning you pay no attorney fees or costs unless we recover compensation for your family. Our firm is led by Tommy Hastings, a board-certified trial lawyer and a 2025 inductee into the American Board of Trial Advocates (ABOTA), an elite group of trial lawyers. Tommy has over two decades of experience helping families manage the aftermath of medical errors. We believe that holding negligent providers accountable is one of the most effective ways to prevent the same thing from happening to another family.
Contact us today for a free, confidential case evaluation. Let us help you find the answers you deserve.
Frequently Asked Questions About Polyhydramnios Mismanagement in Arizona

Key Polyhydramnios Mismanagement Terms:
- Polyhydramnios (hydramnios)
- A pregnancy complication where there is an excessive amount of amniotic fluid surrounding the baby in the uterus. In a medical malpractice case involving missed or delayed diagnosis, this condition matters because doctors have a duty to monitor fluid levels through ultrasound and investigate the underlying cause, as untreated polyhydramnios can lead to serious complications like umbilical cord prolapse, placental abruption, and oxygen deprivation that may cause permanent injury to the baby.
- Uterine overdistension
- A condition where the uterus becomes overly stretched, typically caused by excessive amniotic fluid (polyhydramnios) or carrying multiples. In the context of polyhydramnios mismanagement, this overdistension increases the risk of premature labor, placental problems, and abnormal fetal positioning, all of which require careful medical monitoring and may support a malpractice claim if the healthcare provider failed to recognize or address these dangers.
- Amniotic fluid index (AFI)
- A measurement technique used during ultrasound to assess the amount of amniotic fluid in the uterus by dividing the uterus into four sections and adding up the depth of the deepest fluid pocket in each section. In a polyhydramnios case, an elevated AFI (typically above 24-25 centimeters) should alert the doctor to investigate further and consider treatment, and failure to properly measure or respond to an abnormal AFI may constitute a breach of the standard of care.
- Single deepest pocket (SDP/SDVP)
- An alternative ultrasound method for measuring amniotic fluid that identifies and measures only the single deepest vertical pocket of fluid in the uterus, rather than measuring all four quadrants. This method is considered by some studies to be more accurate than AFI for diagnosing polyhydramnios, with a measurement over 8 centimeters typically indicating excess fluid, and the choice of measurement technique and interpretation of results can be relevant in determining whether a doctor met the standard of care.
- Macrosomia
- A condition where a baby is significantly larger than average at birth, typically weighing more than 8 pounds 13 ounces (4,000 grams) or 9 pounds 15 ounces (4,500 grams), depending on the definition used. In polyhydramnios cases, macrosomia is both a potential cause of excess fluid and a risk factor that doctors should recognize and monitor for, as it increases the likelihood of birth complications including shoulder dystocia, and failure to identify and properly manage a large baby may support a medical malpractice claim.
- Fetal malposition (breech presentation)
- A situation where the baby is not in the normal head-down position for delivery, with breech presentation specifically referring to when the baby’s buttocks or feet are positioned to come out first. Polyhydramnios increases the risk of malposition because the excess fluid allows the baby to move more freely and fail to settle into the proper position, and doctors have a duty to detect these abnormal positions through examination and ultrasound so they can plan for a safer delivery method, such as cesarean section when necessary.
- Umbilical cord prolapse
- A rare but life-threatening emergency where the umbilical cord slips through the cervix and into the birth canal ahead of the baby, which can cut off the baby’s oxygen supply when the cord becomes compressed. In polyhydramnios cases, the excess amniotic fluid significantly increases the risk of cord prolapse, especially when the water breaks, and a doctor’s failure to recognize this danger, monitor appropriately, or deliver the baby promptly when prolapse occurs can constitute negligence resulting in brain damage or death.
- Placental abruption
- A serious pregnancy complication where the placenta partially or completely separates from the inner wall of the uterus before delivery, cutting off oxygen and nutrients to the baby. In the context of polyhydramnios mismanagement, rapid decompression of excess fluid (such as when the water breaks suddenly or during poorly performed amnioreduction) can trigger abruption, and medical providers must recognize this risk and take steps to prevent sudden fluid loss or respond immediately when abruption occurs.
- Amnioreduction (therapeutic amniocentesis)
- A medical procedure where a needle is inserted through the mother’s abdomen into the uterus to drain excess amniotic fluid in cases of severe polyhydramnios. While this treatment can relieve dangerous pressure and reduce complications, it carries risks including infection, premature labor, placental abruption, and injury to the baby, so negligent performance of this procedure—such as removing fluid too quickly, using improper technique, or failing to monitor the mother and baby afterward—may form the basis of a malpractice claim.
- Indomethacin
- A medication (a type of nonsteroidal anti-inflammatory drug) sometimes used to treat polyhydramnios by reducing the amount of urine the fetus produces, thereby decreasing amniotic fluid levels. While it can be effective, indomethacin carries significant risks, including premature closure of an important fetal blood vessel called the ductus arteriosus, which can cause heart and lung problems, so doctors must carefully select appropriate cases, monitor the baby closely during treatment, and discontinue use if complications arise—failure to do so properly may constitute improper medical intervention.
- Polyhydramnios | NCBI Bookshelf
- Polyhydramnios at Term in Gestational Diabetes Should We Be Concerned? | PubMed Central
- Causes, management and outcomes of polyhydramnios at a secondary level hospital in Cape Town, South Africa | PLOS ONE
- Indomethacin induced ductus arteriosus closure in midgestation fetus | PubMed Central
- 12-563 Necessary elements of proof | Arizona Legislature
- Pediatric Life Care Planning Best Practices for Supporting Children with Disabilities | Medical and Life Care Consulting Services
Get Answers Today
If you think that medical negligence, a dangerous drug, or a failed medical product caused harm to you or someone you love, our team is standing by to offer guidance. We’ll explain your options under current laws and help you move forward with clarity and understanding. Case reviews are free and 100% confidential.
