

Arizona Infant Intubation Injury Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: May 6, 2026
Neonatal intubation and mechanical ventilation are time sensitive interventions where small errors can cause severe and lasting harm. This topic involves the NICU standard of care for airway management, the difference between a defensible decision not to intubate and negligent execution, and the ways oxygen deprivation or improper ventilation settings can injure a newborn. It also addresses how liability may extend beyond an individual clinician to a hospital or a device manufacturer when systems or equipment fail. If you or a loved one were harmed or worse due to neonatal intubation or ventilation negligence in Arizona, contact Hastings Law Firm for a free, confidential case review.

Protecting Arizona Families After Neonatal Ventilation Negligence
What You Should Know About Neonatal Ventilation Negligence Claims in Arizona:
- Lifelong disability can result when neonatal intubation is delayed, misplaced, or not confirmed, because even brief oxygen deprivation can cause irreversible brain injury.
- Serious harm can occur even when oxygen levels look normal, because overventilation can drive carbon dioxide too low and reduce cerebral blood flow.
- Liability can extend beyond a single clinician, because hospitals may share responsibility for staffing, protocol, or supervision failures.
- Product related harm can change who is responsible, because defective or recalled intubation devices may shift liability toward a manufacturer.
- Disputes often turn on whether the event was a reasonable judgment call or a preventable technical error during the procedure.
- Recovery options can be shaped by the type of damages available, including economic, non economic, punitive, and wrongful death damages.
- Financial recovery can be substantial when long term care is needed, because Arizona does not cap economic damages in medical malpractice cases.
- Key evidence can be lost over time, because medical records, ventilator data, and monitoring trends can be central to understanding what happened.

A Healthcare Focused Law Firm
When a newborn needs emergency breathing support, every second of care matters. Parents trust that the medical team in the NICU will follow established safety protocols to protect their baby’s airway and prevent oxygen deprivation, a condition known as hypoxia, where the brain and organs do not receive enough oxygen.
If your child was harmed during or after intubation, feeling overwhelmed is a natural response. These questions are valid. An Arizona infant intubation injury lawyer at Hastings Law Firm, a practice dedicated exclusively to medical negligence litigation, can review your child’s medical records, identify where protocols may have failed, and explain your legal options. Contact us for a free, confidential case evaluation to take the first step toward understanding what happened.
Legal Standard of Care for Infant Intubation in Arizona
The standard of care for neonatal intubation requires medical providers to follow established protocols for airway management, including proper tube selection, timely execution, and continuous monitoring of vital signs. When a provider fails to meet this duty of care, the resulting harm may support a medical malpractice claim.
In the NICU, the standard of care refers to the level of treatment a reasonably competent medical professional would provide under similar circumstances. The Neonatal Resuscitation Program (NRP) largely defines the standard for neonatal airway management. These evidence-based guidelines outline how clinicians should evaluate and respond to a newborn in respiratory distress. The NRP algorithm published in PubMed Central provides a concise flow chart for delivery room resuscitation, including when intubation should be initiated and how it should be confirmed.
Timely intubation is critical because even brief periods without adequate oxygen can cause irreversible injury. When a baby cannot breathe effectively on their own, a clinician may need to place an endotracheal tube (ETT). This is a small breathing tube inserted through the mouth or nose into the trachea to deliver oxygen directly to the lungs. Delays in placing or confirming this tube can lead to prolonged oxygen deprivation and potential brain damage.
Medical experts help establish what a prudent neonatal provider would have done in the same situation. We work with these specialists to reconstruct the clinical timeline and determine whether the care team met or fell short of the expected standard.
Key elements of the neonatal intubation standard of care include:
- Recognizing signs of respiratory failure and starting treatment quickly
- Selecting the correct size endotracheal tube based on the infant’s weight and gestational age
- Confirming proper tube placement using capnography and clinical assessment
- Continuously monitoring oxygen saturation, heart rate, and chest rise after intubation
- Having backup airway equipment immediately available in the resuscitation area
Decision Not to Intubate vs. Negligent Execution
There is an important legal distinction between a physician’s medical judgment call to delay intubation and a technical failure in performing the procedure. A decision to continue less invasive ventilation support, such as bag-mask ventilation, may be clinically appropriate if the infant is responding. That is a judgment call and is not automatically medical negligence.
Negligent execution involves errors in how the procedure is carried out. Placing the tube in the wrong location, using an improperly sized tube, or failing to verify placement are technical failures that can constitute a breach of the standard of care. When we investigate these cases, we examine the records and ventilator data to determine whether the issue was a defensible clinical decision or a preventable procedural error.

Common Causes of Preventable Airway Injuries in the NICU
Preventable airway injuries often stem from technical errors such as esophageal intubation, using the wrong size endotracheal tube, or failing to secure the tube properly, leading to accidental extubation, where the tube becomes dislodged from the airway after placement. In some cases, systemic issues like hospital negligence or insufficient staffing of nurses can also contribute to these preventable errors.
One of the most dangerous errors is esophageal intubation, which occurs when the breathing tube is placed into the esophagus (the food pipe) instead of the trachea (the windpipe). When this happens, oxygen is delivered to the stomach rather than the lungs. The stomach may distend, further compressing the lungs and making ventilation even more difficult. If the misplacement is not identified and corrected quickly, the infant can suffer severe oxygen deprivation within minutes.
Proper use of monitoring equipment should catch this error almost immediately, but failures in reading or responding to that data still occur. Reliance solely on clinical signs like chest wall movement can be misleading, as air entering the stomach can mimic chest rise.
Common technical errors that can lead to neonatal airway injury include:
- Tube misplacement: Inserting the ETT into the esophagus or advancing it too far into one bronchus, ventilating only one lung
- Incorrect tube size: Using a tube that is too large, causing tracheal trauma, or too small, resulting in inadequate ventilation
- Failure to secure the tube: Leading to accidental extubation during routine repositioning or transport
- Monitoring failures: Not reading capnography data or ignoring vital sign changes that indicate the tube is not functioning properly
- Delayed response: Failing to act when alarms signal desaturation or airway obstruction
Equipment defects can also cause harm. Defective or recalled intubation devices may malfunction during a procedure. If that happens, liability may shift from the clinical team to the manufacturer.
The U.S. Food and Drug Administration’s Class 1 Device Recall of Medline intubation products is one example of how defective equipment can create risk in the NICU. An infant intubation malpractice lawyer in Arizona can help determine whether a product defect, clinical negligence, or both contributed to the injury.
Risks of Unqualified Trainees Performing Procedures
In teaching hospitals, residents and medical students sometimes perform neonatal intubation as part of their training. This is not inherently unsafe, but it does require direct supervision by an experienced attending physician.
When a trainee performs a complex procedure like neonatal intubation without adequate oversight, and an injury results, the hospital and supervising physician may share liability for that outcome. This failure of oversight can be the basis of a medical malpractice claim. We examine training logs, supervision records, and attending documentation to evaluate whether proper safeguards were in place.

The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

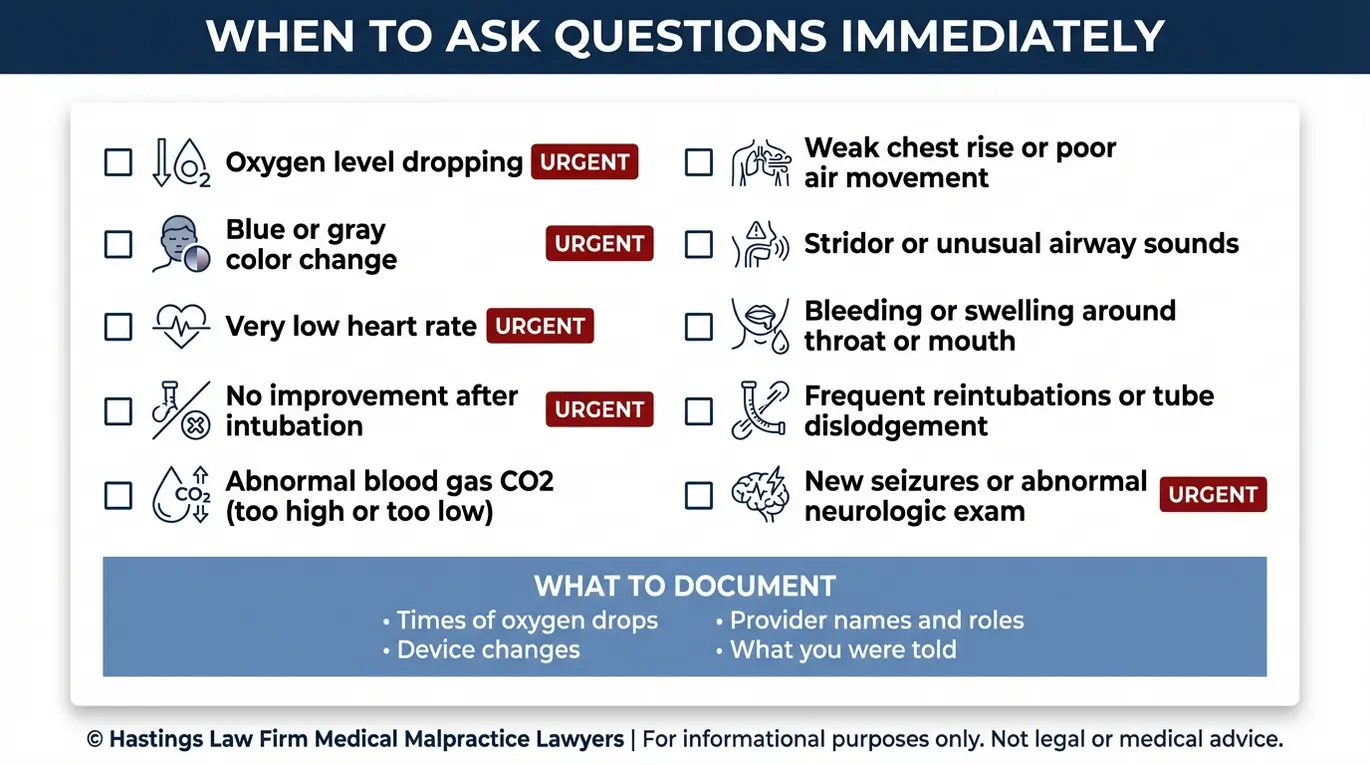
Signs of Respiratory Distress and Intubation Trauma
Signs of intubation trauma or failure include dropping oxygen saturation levels, physical damage to the trachea or vocal cords, and abnormal blood gas readings that indicate poor ventilation. Recognizing these signs early is essential because delays in corrective action can lead to lasting harm.
Immediate clinical signs that may indicate a failed or traumatic intubation include cyanosis, a bluish discoloration of the skin caused by low oxygen, and bradycardia, an abnormally slow heart rate. These are red flags that the infant is not receiving adequate oxygen and that the airway may be compromised.
Physical trauma from intubation can present as swelling, bruising, or bleeding in the throat area. Damage to the vocal cords, tracheal perforation, or soft tissue injury can result from repeated insertion attempts or improper technique. These injuries may be documented in post-procedure imaging or noted during later evaluations.
Neurological impact is the most serious concern. Prolonged oxygen deprivation can cause hypoxic-ischemic encephalopathy (HIE), a form of brain damage that may lead to cerebral palsy or other permanent disabilities. The longer the brain goes without adequate oxygen, the greater the risk of irreversible injury.
| Warning Sign | What It May Indicate |
|---|---|
| Falling oxygen saturation (SpO2) | Tube misplacement or obstruction |
| Cyanosis (blue skin) | Inadequate oxygenation |
| Bradycardia (low heart rate) | Vagal response or severe hypoxia |
| Swelling or bleeding in the throat | Physical trauma from intubation attempts |
| Abnormal arterial blood gas (ABG) values | Poor gas exchange; possible ventilation failure |
| Abnormal capnography readings | Tube not in the trachea or ventilator malfunction |
An arterial blood gas (ABG) test measures oxygen and carbon dioxide levels in the blood. Capnography, also called end-tidal CO2 monitoring, tracks carbon dioxide levels in exhaled breath. Both tools are standard methods for confirming that ventilation is working. When these readings are abnormal and the care team does not respond appropriately, it can form the basis of a negligence claim.
Understanding Overventilation and Hypocarbia Risks
Not all ventilation injuries come from too little oxygen. Overventilation, which means delivering breaths at too high a rate or volume through mechanical ventilation, can drive carbon dioxide levels dangerously low. This condition is called hypocarbia. When CO2 drops too far, blood vessels in the brain constrict, reducing cerebral blood flow. In a fragile newborn, this reduction can cause brain damage even when oxygen levels appear normal on the monitor.
This type of injury is difficult for parents to understand because the ventilator appears to be working. But the settings may be wrong, and the resulting chemical imbalance in the blood can quietly injure the brain. We examine ventilator logs, blood gas trends, and nursing documentation to evaluate whether ventilation settings were managed appropriately.
Liability and Compensation for Birth Airway Injuries
Liability for a birth airway injury may extend to the hospital for staffing or protocol failures, the individual physician for procedural errors, or the manufacturers of defective medical devices. In many cases, more than one party bears responsibility. Medical malpractice cases involving infants are legally complex because the standard of care involves specialized neonatal protocols. A thorough investigation must determine if the injury resulted from a momentary lapse in judgment or a systemic failure to follow safety rules.
Potential defendants include the neonatologist who managed the airway and nursing staff responsible for monitoring. Other parties may include respiratory therapists and the hospital itself for systemic issues like inadequate staffing or lack of proper equipment. Our founder, Tommy Hastings, is Board Certified in Personal Injury Trial Law and an inductee into the American Board of Trial Advocates (ABOTA), and he understands how to build a case that clearly shows where medical standards were not followed. In complex NICU environments, determining liability often requires distinguishing between individual provider errors and systemic facility failures.
Once we establish liability, families may recover compensation in several categories:
- Economic damages: These cover measurable financial losses, including past and future medical bills and therapy costs. They also include life care planning for children who need ongoing support, adaptive equipment, and future lost earning capacity. Calculations often include the expense of life care plans covering 24-hour nursing, home modifications, and specialized therapies, which can reach into the millions over a lifetime.
- Non-economic damages: These compensate for harm that does not carry a price tag, such as pain and suffering, physical impairment, and the emotional toll on the family. While no amount of money can undo the injury, these damages acknowledge the profound alteration of the child’s quality of life.
- Punitive damages: In rare cases involving extreme or reckless conduct, Arizona courts may award punitive damages to penalize the wrongdoer and discourage similar behavior. This is most common in cases where a provider was under the influence of drugs or where the hospital knowingly allowed an unsafe practice to continue.
- Wrongful death damages: If an infant does not survive injuries caused by negligent intubation or ventilation, the family may pursue a wrongful death claim. A wrongful death claim can provide financial stability for the grieving family and hold the negligent parties publicly accountable.
Arizona does not cap economic damages in medical malpractice cases, which means families can pursue the full cost of lifetime care for a child with serious disabilities.
Contact the Arizona Birth Injury Attorneys at Hastings Law Firm Today for Help
If your child suffered harm during intubation or mechanical ventilation, you deserve answers. At Hastings Law Firm, our medical-legal team, which includes nurse practitioners and former defense attorneys who previously defended hospital systems, conducts a thorough review of every record and clinical decision to determine what went wrong.
We believe that holding negligent providers accountable is one of the most meaningful ways to prevent the same harm from happening to another family. That principle drives every case we take.
There is no cost to get started. As an Arizona infant intubation injury lawyer, we work on a contingency fee basis, meaning you pay no attorney fees unless we recover compensation for your family. Contact us today for a free, confidential case evaluation. Let us help you find the answers you deserve.
Frequently Asked Questions About Infant Intubation Injury in Arizona

Key Infant Intubation Injury Terms:
- Oxygen deprivation (hypoxia)
- A dangerous condition where the body or brain does not receive enough oxygen. In newborns, even brief periods of oxygen deprivation during or after intubation can cause permanent brain damage, including cerebral palsy or hypoxic-ischemic encephalopathy (HIE). In medical malpractice cases, proving that negligent intubation caused hypoxia is key to establishing liability.
- Neonatal Resuscitation Program (NRP)
- A nationally recognized training program developed by the American Academy of Pediatrics that establishes guidelines for resuscitating and stabilizing newborns in distress. Healthcare providers in delivery rooms and NICUs are expected to follow NRP protocols when intubating infants. Deviation from NRP standards can be evidence of a breach of the medical standard of care in a malpractice claim.
- Endotracheal tube (ETT)
- A flexible plastic tube inserted through a newborn’s mouth or nose into the trachea (windpipe) to deliver oxygen directly to the lungs when the baby cannot breathe adequately on their own. Proper placement and securement of the ETT is critical; errors in insertion or positioning can lead to oxygen deprivation and serious injury.
- Esophageal intubation
- A serious medical error that occurs when the endotracheal tube is mistakenly inserted into the esophagus (the tube leading to the stomach) instead of the trachea (windpipe). This prevents oxygen from reaching the lungs and can cause rapid oxygen deprivation, brain damage, or death if not immediately recognized and corrected. In malpractice cases, esophageal intubation is often considered preventable with proper technique and monitoring.
- Accidental extubation
- The unintended removal or dislodgement of the endotracheal tube from a baby’s airway. This can happen due to inadequate securement of the tube, improper handling during care, or failure to monitor tube placement. Accidental extubation interrupts oxygen delivery and may require emergency re-intubation to prevent harm. It may constitute negligence if it results from a failure to follow proper protocols.
- Capnography (end-tidal CO2/EtCO2 monitoring)
- A monitoring technique that measures the amount of carbon dioxide exhaled with each breath to confirm that the endotracheal tube is correctly placed in the trachea and that the baby is breathing adequately. Capnography provides immediate feedback; a lack of CO2 detection indicates the tube may be in the esophagus or dislodged. Failure to use or respond to capnography readings can be evidence of substandard care in intubation injury cases.
- Arterial blood gas (ABG)
- A blood test that measures the levels of oxygen, carbon dioxide, and acidity (pH) in the blood, typically drawn from an artery. In the NICU, ABG results help clinicians assess how well a baby’s lungs are working and whether the ventilator settings are appropriate. Abnormal ABG values can indicate complications from intubation or ventilation, and failure to act on concerning results may support a claim of medical negligence.
- Overventilation
- Providing too much mechanical breathing support or delivering breaths too rapidly or forcefully to an intubated infant. Overventilation can cause trauma to fragile lung tissue and lead to dangerously low levels of carbon dioxide in the blood (hypocarbia), which restricts blood flow to the brain and increases the risk of brain injury. In malpractice claims, overventilation may be evidence of improper ventilator management.
- Hypocarbia
- An abnormally low level of carbon dioxide in the blood, often caused by overventilation. In newborns, hypocarbia causes blood vessels in the brain to constrict, reducing oxygen delivery to brain tissue and increasing the risk of brain damage, bleeding, or developmental problems such as cerebral palsy. Failure to monitor and prevent hypocarbia during mechanical ventilation can be a basis for a medical malpractice claim.
- 12-502 Effect of minority or insanity | Arizona State Legislature
- 12 542 Injury to person injury when death ensues injury to property conversion of property forcible entry and forcible detainer two year limitation | Arizona Legislature
- Neonatal resuscitation program algorithm with timeline A concise flow chart for delivery room resuscitation | PubMed Central
- Class 1 Device Recall Medline | U.S. Food and Drug Administration
Get Answers Today
If you think that medical negligence, a dangerous drug, or a failed medical product caused harm to you or someone you love, our team is standing by to offer guidance. We’ll explain your options under current laws and help you move forward with clarity and understanding. Case reviews are free and 100% confidential.
