

Arizona Low PAPP-A IUGR Negligence Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: May 6, 2026
Low PAPP A in early pregnancy can signal placental problems that raise the risk of fetal growth restriction and serious outcomes. When that warning sign is missed or not acted on, a pregnancy that needed close surveillance can proceed without the monitoring that helps detect decline in time. The result can be oxygen deprivation, permanent brain injury, a birth injury, or worse. Understanding what the screening showed and how the care plan responded can clarify whether the standard of care was met. If you or a loved one were harmed or worse due to low PAPP A IUGR negligence in Arizona, contact Hastings Law Firm for a free, confidential case review.

Seeking Justice for Preventable Birth Injuries in Arizona
What You Should Know About Prenatal Screening Oversight Claims in Arizona:
- Severe harm can follow when low PAPP A is not treated as a high risk finding because fetal growth restriction and placental failure can progress without timely detection.
- Permanent neurological injury can result when unmanaged fetal growth restriction leads to prolonged oxygen deprivation.
- Stillbirth can occur when placental function declines and monitoring is not frequent enough to detect the final deterioration.
- Options can narrow when a pregnancy is not reclassified as high risk because enhanced surveillance may not be put in place.
- Preventable injury can be linked to missed or delayed growth surveillance because serial ultrasounds and related testing are used to track growth velocity and fetal well being.
- Catastrophic outcomes can become more likely when abnormal Doppler findings are not acted on because absent or reversed end diastolic flow signals immediate danger.
- Liability disputes can turn on whether the fetus was constitutionally small because proportional growth patterns differ from declining growth percentiles.
- Proof can depend on objective placental findings because pathology may show infarction, calcification, or clots consistent with placental insufficiency.
- Causation can be contested when imaging is misread because asymmetrical growth patterns may be overlooked.
- Evidence can become harder to secure over time because key records like fetal monitoring strips and placental pathology reports may deteriorate or be difficult to obtain.

A Healthcare Focused Law Firm
When prenatal screening reveals a warning sign like low PAPP-A, that result carries meaning. It signals a need for closer monitoring, more frequent imaging, and a heightened awareness of the risks to your baby. If those steps were not taken, and your child suffered a birth injury or was stillborn, you deserve to know whether the care you received met the standard your pregnancy required.
An Arizona low PAPP-A IUGR negligence lawyer can help you understand what went wrong and whether your provider’s response to known risk factors fell short. At Hastings Law Firm, founded by board-certified trial attorney Tommy Hastings, our legal and medical team reviews prenatal records, screening results, and monitoring timelines to determine if negligence contributed to your child’s injury.
If you have questions about what happened during your pregnancy, we can review your records and explain your options during a free, confidential consultation.
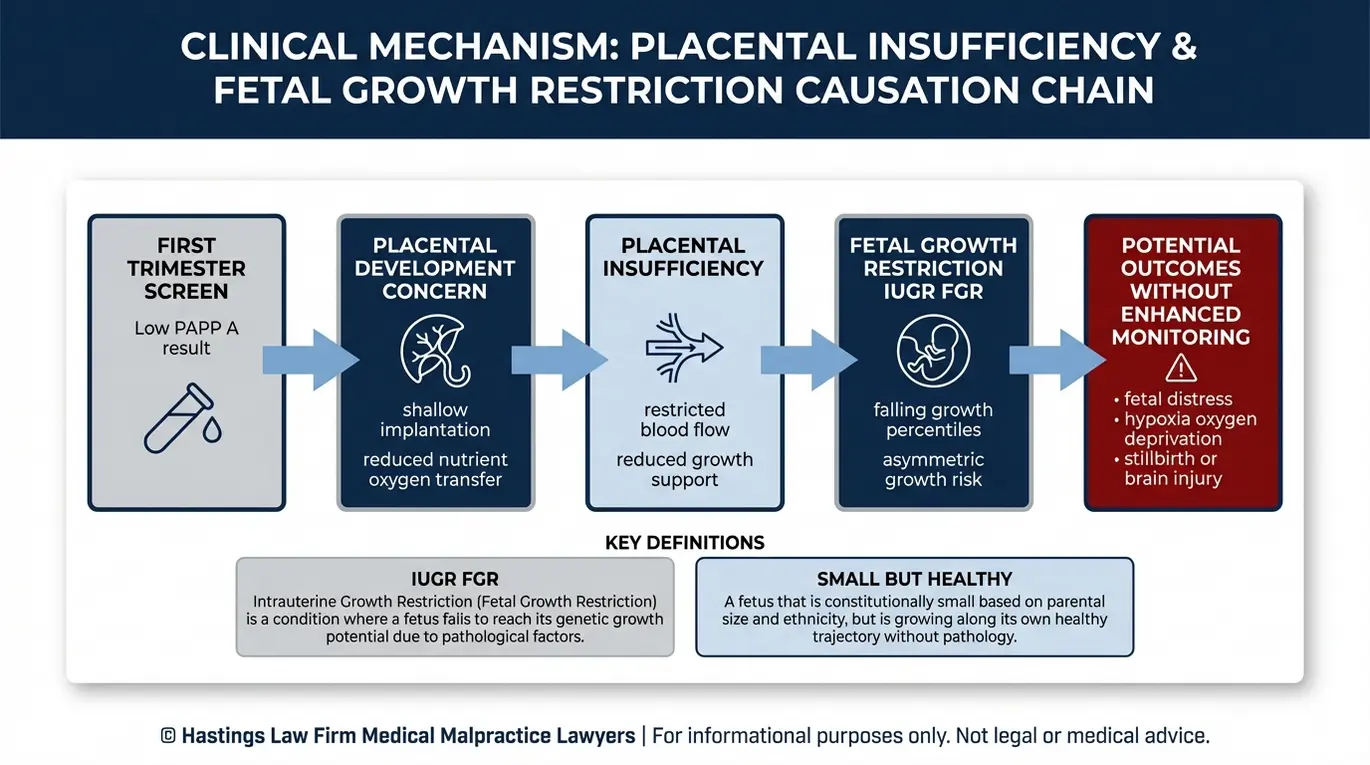
The Critical Link Between Low PAPP-A and Intrauterine Growth Restriction
Low PAPP-A is a protein marker that, when found in low levels during the first trimester, indicates poor placental development and a significantly higher risk for Intrauterine Growth Restriction (IUGR), preeclampsia, and stillbirth, requiring enhanced monitoring protocols. These findings call for enhanced prenatal screening and ongoing surveillance throughout the pregnancy to ensure the fetus continues to receive adequate oxygen and nutrients despite the placental challenges.
Key definitions in these cases include:
- Pregnancy-Associated Plasma Protein A (PAPP-A): A protein produced by the placenta early in pregnancy. Its role is to help regulate the insulin-like growth factors that allow the placenta to implant deeply into the uterine wall and develop the blood vessel network that will nourish the baby for the next nine months. When PAPP-A levels are low on a first-trimester blood draw, it often indicates that this implantation process is shallow or incomplete, leading to a condition known as placental insufficiency.
- Intrauterine Growth Restriction (IUGR): A condition, also referred to as fetal growth restriction (FGR), where the fetus is not reaching its expected growth potential. This is distinct from a baby that is simply small due to parental stature. A baby with IUGR is being deprived of adequate resources because the placenta cannot keep up with the metabolic demands of the growing pregnancy.
Placental insufficiency is the underlying mechanism connecting the lab result to the injury. When the placenta fails to remodel the uterine arteries effectively, it creates a high-resistance environment for blood flow. As the pregnancy progresses and the baby requires more energy to grow, this compromised organ reaches a breaking point. The fetus may stop growing or begin to conserve energy by reducing movement and slowing its heart rate.
A study published in PubMed Central examining first-trimester serum levels of β-hCG and PAPP-A confirmed the value of these markers as screening tools for predicting IUGR. When providers identify low PAPP-A, it should trigger a shift in how the entire pregnancy is managed.
The risks of unmanaged IUGR are serious:
- Chronic hypoxia: Prolonged oxygen deprivation causes metabolic acidosis in the fetus. Over time, this can lead to permanent brain injury, including cerebral palsy and periventricular leukomalacia (damage to the brain’s white matter).
- Stillbirth: A failing placenta may stop functioning entirely, resulting in fetal death before or during delivery. This often happens quickly if monitoring is not frequent enough to catch the final decline.
- Low birth weight complications: Babies born with IUGR face a higher likelihood of respiratory distress, feeding difficulties, and long-term developmental challenges because their organs were stressed in utero.
An Arizona IUGR malpractice lawyer examines whether the provider recognized the low PAPP-A finding and acted on it. A lawyer for low PAPP-A negligence focuses on the gap between what the screening revealed and what the medical team actually did in response. If your pregnancy was flagged as high-risk due to placental insufficiency but follow-up care was inadequate, a birth injury attorney can help determine whether negligence occurred.
Standard of Care for Managing High-Risk Pregnancies and Fetal Growth
The standard of care for pregnancies with low PAPP-A requires reclassifying the pregnancy as high-risk and implementing a monitoring regimen that includes serial growth ultrasounds, umbilical artery Doppler flow studies, and nonstress tests to track fetal well-being and placental function.
Once a first-trimester screen identifies low PAPP-A, the treating obstetrician has an obligation to adjust the care plan. The pregnancy is no longer routine. Accepted medical guidelines, including those outlined by Guideline Central’s clinical summary on fetal growth restriction, establish a clear high-risk pregnancy protocol for how these pregnancies should be managed to prevent injury.
Serial Growth Ultrasounds
Standard practice calls for serial growth ultrasounds, typically every three to four weeks beginning around 28 weeks of gestation. These ultrasounds measure the estimated fetal weight (EFW) and plot it against established growth curves. The objective is to track the growth velocity.
An Arizona prenatal negligence lawyer will review your records to determine whether these growth scans were ordered and whether the results were interpreted correctly to catch this “falling off the curve” phenomenon.
Umbilical Artery Doppler Flow Studies
Umbilical artery Doppler flow studies, which measure the resistance of blood flow through the umbilical cord, are a direct indicator of placental function. In a healthy pregnancy, blood flows easily from the placenta to the baby even when the fetal heart is relaxing (diastole). Placental insufficiency causes increased resistance, forcing the fetal heart to work harder.
In severe cases, doctors may observe absent or reversed end-diastolic flow, a finding that indicates the baby is in immediate danger of heart failure or stillbirth. This is the point where delivery discussions should begin. A medical malpractice attorney for missed IUGR will evaluate whether Doppler studies were ordered and whether abnormal findings prompted timely action.
Referral to Maternal-Fetal Medicine
The standard of care also requires general OB-GYNs to recognize the limits of their expertise. When a pregnancy involves low PAPP-A and suspected fetal growth restriction, referral to a maternal-fetal medicine specialist (MFM) is often required. MFM specialists have the training and equipment to perform advanced monitoring, including biophysical profiles that assess fetal movement, tone, breathing, and amniotic fluid levels. These detailed assessments provide a more granular view of fetal health than standard checks.
A lawyer for high-risk pregnancy errors will look at whether a referral was made, how quickly it happened, and whether the MFM’s recommendations were followed.
| Screening Method | Frequency / Timing | Purpose |
|---|---|---|
| Serial growth ultrasounds | Every 3–4 weeks starting at ~28 weeks | Track estimated fetal weight and growth trends |
| Umbilical artery Doppler flow studies | As clinically indicated; more frequent with abnormal findings | Assess placental blood flow resistance |
| Nonstress test (NST) | Weekly or biweekly in the third trimester | Monitor fetal heart rate patterns for signs of distress |
| Biophysical profile (BPP) | As indicated by NST or Doppler results | Evaluate fetal movement, tone, breathing, and amniotic fluid |
| MFM referral | Upon identification of high-risk factors | Provide specialized oversight for complex pregnancies |
When any of these steps are skipped or delayed, the consequences can be catastrophic. Our team at Hastings Law Firm, which includes former defense attorneys and board-certified patient advocates, knows exactly where to look in the medical records to identify these gaps.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Identifying Negligence and Failures in Diagnosing or Monitoring IUGR
Negligence in IUGR cases often occurs when providers dismiss low PAPP-A findings, fail to order third-trimester growth scans, misinterpret ultrasound data, or delay cesarean section delivery despite evidence of fetal distress or halted growth. An Arizona birth injury lawyer examines each of these potential failure points during a medical malpractice investigation to determine where the standard of care was breached.
According to the American Academy of Family Physicians’ clinical review on fetal growth restriction, the tools to identify and manage IUGR are well-established. The question in a negligence case is whether those tools were used. Our investigation typically focuses on four key areas.
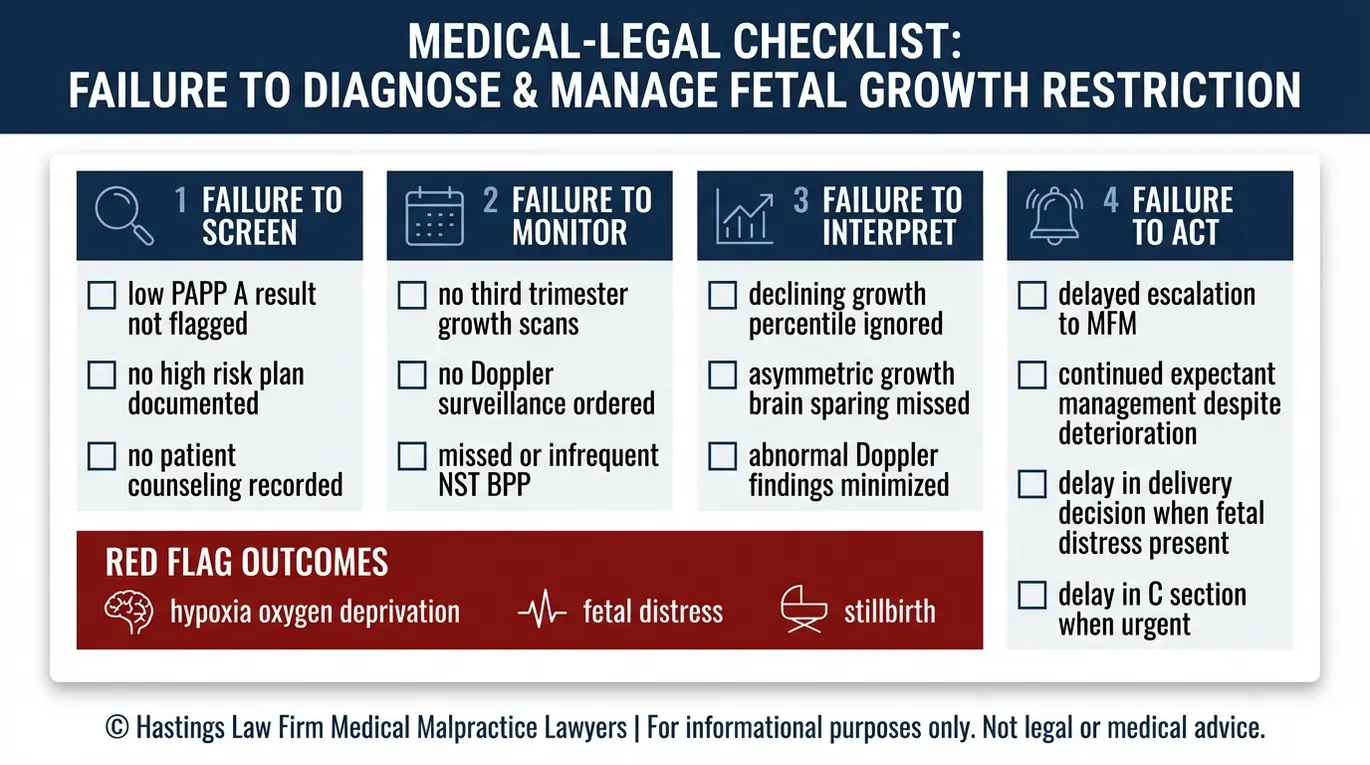
The Four Points of Failure
- Failure to screen: The first failure can occur at the very beginning, when a provider receives a low PAPP-A result from the first-trimester screen but does not flag the pregnancy as high-risk. In some cases, the result may be noted in the chart but never discussed with the patient or incorporated into the care plan. When suing for IUGR negligence, this is often the earliest point where the chain of errors begins. This omission deprives the medical team of the critical baseline data needed to effectively manage the third trimester.
- Failure to monitor: Even when the risk is identified, negligence can occur if the provider does not follow through with serial growth ultrasounds, which track the estimated fetal weight over time, or Doppler flow studies. A gap in monitoring during the third trimester is a common finding in medical negligence cases involving IUGR. If weeks pass without an updated growth assessment, warning signs can go undetected. Without these data points, the fetus’s decline remains invisible to the medical team until it is too late.
- Failure to interpret: Ordering the right tests is only half the obligation. The data must be read correctly. Asymmetrical IUGR, sometimes called the “brain-sparing” effect, occurs when the baby’s body redirects blood flow to the brain at the expense of the abdomen and limbs. This creates a pattern where the head circumference measures normally, but the abdominal circumference falls behind. If a radiologist or obstetrician misses this subtle asymmetry, the baby may be incorrectly labeled as developing on track.
- Failure to act: The most consequential failure is a delay in delivery when the evidence shows the placenta is failing. When Doppler studies reveal absent or reversed end-diastolic flow, or when growth has plateaued across consecutive ultrasounds, the standard of care may require an emergency C-section. Waiting too long exposes the baby to oxygen deprivation, which can cause permanent brain injury or stillbirth. A failure to diagnose IUGR attorney will review the timing of delivery decisions against the clinical data available to the provider at the time.
The four points of failure in these cases usually involve deviations from standard monitoring protocols. At Hastings Law Firm, our medical-legal team reconstructs the full timeline to identify every point where the care deviated from what the pregnancy required.
Overcoming Common Defenses in Fetal Growth Restriction Lawsuits
Defense attorneys frequently argue that the infant was “constitutionally small” rather than pathologically restricted to avoid liability, a claim that can be refuted by analyzing placental pathology reports and Doppler history. An Arizona medical malpractice lawyer with experience in these cases knows how to challenge this defense using objective medical evidence.
The “Constitutionally Small” Defense
A constitutionally small fetus follows a consistent growth curve because it is genetically predisposed to be smaller than average while remaining healthy. The baby’s growth is proportional, and the placenta is functioning normally. This is fundamentally different from a baby with IUGR, whose small size reflects deprivation, not genetics.
The distinction matters because if the defense can convince a jury that the baby was simply small, there is no negligence. An IUGR negligence attorney challenges this argument by examining growth velocity. A constitutionally small baby stays on their curve. A baby with fetal growth restriction shows declining percentiles, falling off the curve over time as the placenta deteriorates.
Defense vs. Reality
- Defense Claim: The defense will argue the baby’s small size was a fixed genetic trait (“small parents make small babies”) and that no amount of monitoring would have changed the outcome.
- Medical Reality: Placental pathology reports often reveal infarction (dead tissue), calcification, and clots, proving the organ was failing. Also, growth charts typically show the baby stopped growing in the final weeks, directly contradicting the genetic argument.
The Importance of Placental Pathology
One of the most powerful pieces of evidence in a fetal growth restriction injury case is the placental pathology report. After delivery, the placenta can be examined under a microscope for signs of infarction, calcification, and vascular abnormalities. A healthy placenta is spongy and vascular; an IUGR placenta is often gritty, small, and filled with areas of poor blood flow. These findings directly validate the low PAPP-A warning from the first trimester and confirm that the placenta was not functioning properly.
Research published in PubMed Central on predicting adverse perinatal outcomes in small-for-gestational-age fetuses underscores the value of combining clinical imaging with pathological data to distinguish between a healthy small baby and one suffering from true growth restriction. A lawyer for fetal growth restriction injury in Phoenix will work with expert witnesses who can present this evidence in a way a jury can understand.
The “Brain-Sparing” Phenomenon
Asymmetrical IUGR provides some of the strongest evidence against the “constitutionally small” defense. When a baby’s body is deprived of adequate oxygen and nutrients, the autonomic nervous system redirects blood flow to vital organs, primarily the brain and heart, at the expense of the liver, kidneys, and limbs. This results in a head that measures normally while the abdominal circumference lags significantly.
This is not a genetic trait; it is a desperate physiological survival response to starvation and placental insufficiency. Expert testimony from maternal-fetal medicine specialists and neonatologists can explain this phenomenon to a jury and connect it directly to the failure to monitor or act.
An Arizona medical malpractice lawyer at Hastings Law Firm builds these cases by pairing the clinical evidence with qualified experts who can clearly explain what the data shows and what should have been done differently. Hypoxia-related injuries, including cerebral palsy and other permanent neurological damage, are the direct downstream consequences of unaddressed IUGR. Proving damages in these cases requires a thorough accounting of the child’s lifetime care needs, along with the pain and suffering endured by the child and family.
Contact the Arizona Birth Injury Attorneys at Hastings Law Firm Today for Help
When prenatal screening identifies a risk and the medical team does not respond, the injury that follows is not just a medical event. It is a violation of trust. You relied on your providers to protect your baby, and you deserve to know whether they met that obligation.
Hastings Law Firm represents Arizona families whose children were harmed by preventable failures in prenatal care. Our team includes in-house medical staff, former defense attorneys, and a national network of expert witnesses who specialize in maternal-fetal medicine and obstetrical standards of care. We handle these cases on a contingency fee basis, which means you pay no attorney fees or costs unless we recover compensation for your family.
If your child suffered a birth injury or you experienced a stillbirth after a low PAPP-A finding was identified during your pregnancy, we want to hear from you. Contact our Phoenix-based Arizona low PAPP-A IUGR negligence lawyer team for a free case evaluation. Let us review your records and help you understand what happened.
Frequently Asked Questions About Low PAPP-A IUGR Negligence in Arizona

Key Low PAPP-A IUGR Negligence Terms:
- Pregnancy-Associated Plasma Protein A (PAPP-A)
- A protein produced by the placenta during pregnancy that can be measured through a blood test, typically in the first trimester. Low levels of PAPP-A serve as an early warning sign that the placenta may not be functioning properly, increasing the risk of growth problems for the baby later in pregnancy. In a medical malpractice case, failure to recognize or act on abnormally low PAPP-A results can constitute negligence if it leads to undiagnosed or unmonitored fetal growth restriction.
- Intrauterine growth restriction (IUGR) / fetal growth restriction (FGR)
- A condition where a fetus does not grow to its expected size during pregnancy, failing to reach its full growth potential due to problems with the placenta, maternal health issues, or other factors. This is different from a baby who is simply small but healthy. IUGR significantly increases risks of oxygen deprivation, stillbirth, and permanent brain injury. In malpractice cases, proving IUGR requires demonstrating that the baby was not just constitutionally small, but was actually being deprived of necessary nutrients and oxygen.
- Placental insufficiency
- A condition where the placenta fails to deliver adequate oxygen and nutrients to the developing fetus. This dysfunction is often signaled by low PAPP-A levels and can lead to intrauterine growth restriction and other serious complications. In medical malpractice claims involving fetal growth problems, proving placental insufficiency is critical to establishing that the baby’s small size was pathological rather than genetic, and that closer monitoring or earlier delivery was medically necessary.
- Umbilical artery Doppler flow studies (including absent or reversed end-diastolic flow)
- Specialized ultrasound tests that measure blood flow through the umbilical cord connecting the baby to the placenta. These studies assess resistance in the umbilical artery to detect whether the baby is receiving adequate oxygen and nutrients. Absent or reversed end-diastolic flow indicates severe placental dysfunction and signals that the baby is at high risk for heart failure, oxygen deprivation, and death. Failure to order these studies when a fetus is at risk for growth restriction, or failure to act on abnormal results, can constitute medical negligence.
- Serial growth ultrasounds
- A series of ultrasound examinations performed at regular intervals throughout pregnancy, typically every three to four weeks, to track whether the fetus is growing appropriately along expected growth curves. For high-risk pregnancies with factors like low PAPP-A, serial ultrasounds are the standard of care for detecting intrauterine growth restriction early. In malpractice cases, failure to order these follow-up scans despite known risk factors can be evidence of negligent monitoring.
- Estimated fetal weight (EFW)
- A measurement calculated from ultrasound readings that estimates how much the fetus weighs at a given point in pregnancy. Healthcare providers use EFW to determine if a baby is growing on track or falling below expected growth percentiles. In cases involving suspected growth restriction, repeated EFW calculations help document whether growth is slowing or stopping. Misinterpretation of EFW data or failure to compare measurements over time can support a claim of negligent diagnosis or monitoring.
- Constitutionally small fetus
- A baby who is small in size due to genetics or family traits rather than from a disease process or placental dysfunction. A constitutionally small fetus is healthy and receiving adequate oxygen and nutrition, just naturally smaller. This is a common defense in growth restriction lawsuits, where healthcare providers argue the baby was always going to be small rather than suffering from true IUGR. Overcoming this defense typically requires evidence such as abnormal Doppler studies, placental pathology, or signs of fetal distress that prove the small size was pathological, not genetic.
- Placental pathology
- The medical examination and analysis of the placenta after delivery to identify abnormalities, disease, or dysfunction. Pathology findings can reveal evidence of chronic insufficiency, infarctions, or other damage that caused the baby to be deprived of oxygen and nutrients during pregnancy. In medical malpractice cases involving fetal growth restriction, placental pathology provides crucial post-birth proof that the placenta was failing and that earlier warnings like low PAPP-A should have prompted more aggressive monitoring and intervention.
- Brain-sparing (asymmetrical IUGR)
- A pattern of growth restriction where the fetus’s head and brain grow at a relatively normal rate while the body and abdomen remain smaller than expected. This occurs because the stressed fetus redirects limited blood flow and oxygen preferentially to protect the brain. Brain-sparing is a sign of fetal distress and chronic oxygen deprivation, not normal genetic variation. In malpractice cases, evidence of asymmetrical growth supports claims that the baby was suffering from placental insufficiency and needed closer monitoring or earlier delivery to prevent permanent injury or death.
- Study of first trimester serum levels of β hCG and PAPP A as a screening test for fetal development of intrauterine growth restriction | PubMed Central
- Fetal Growth Restriction | Guideline Central
- Fetal Growth Restriction Before and After Birth | American Academy of Family Physicians
- Predicting adverse perinatal outcomes in small for gestational age fetuses using MRI ultrasound and clinical data | PubMed Central
- Antenatal Steroids for Women at Risk of Preterm Delivery | University of Cincinnati
Get Answers Today
If you think that medical negligence, a dangerous drug, or a failed medical product caused harm to you or someone you love, our team is standing by to offer guidance. We’ll explain your options under current laws and help you move forward with clarity and understanding. Case reviews are free and 100% confidential.
