

Arizona Infant Delayed Airway Management Lawyer
Written by: Hastings Law Firm | Reviewed by: Tommy Hastings | Updated: July 27, 2026
Delayed or improper airway management during delivery room or NICU resuscitation can leave a newborn without adequate oxygen and cause lasting harm. Standards like the Neonatal Resuscitation Program set expectations for rapid assessment and timely escalation when breathing or heart rate is not adequate. When care teams miss warning signs, fail to prepare equipment, or perform intubation incorrectly, families may face permanent neurological injury, extensive medical needs, and profound disruption to daily life. If you or a loved one were harmed or worse due to delayed newborn airway management in Arizona, contact Hastings Law Firm for a free, confidential case review.
Legal Representation for Newborn Respiratory Injuries in Arizona
What You Should Know About Newborn Respiratory Distress Negligence Claims in Arizona:
- Long term neurological injury can follow when a newborn does not receive timely ventilation or intubation during resuscitation.
- Accountability disputes can turn on whether the error was a failure to intubate when indicated or an improperly performed intubation.
- Options for recovery can be shaped by whether the injury is linked to delayed airway management rather than genetics or infection.
- Additional harm can continue after oxygen is restored because reperfusion injury is described as a secondary wave of damage.
- Separate malpractice exposure can arise when cooling therapy for moderate to severe HIE is not started in time or transfer is delayed.
- Liability can extend beyond the delivering physician because nurses, respiratory therapists, neonatologists, and hospitals may share responsibility.
- Recovery can be limited if action is delayed because evidence can be lost and witness memories can fade over time.
- Compensation can involve lifetime medical care and lost earning capacity because these injuries may require decades of support.
- Objective records can be central because pulse oximetry data and umbilical cord blood gas results can show the timing and severity of oxygen deprivation.
- Future care planning can drive damages because a Life Care Plan is used to project long term costs for a child with brain injury.

A Healthcare Focused Law Firm
When a newborn struggles to breathe and the medical team’s response falls short, the consequences for a family can be permanent. If your child suffered a brain injury or other harm because of a delay in airway management at birth, you are not alone, and you have the right to ask hard questions about what happened in that delivery room or NICU.
At Hastings Law Firm, our team of medical malpractice attorneys, in-house nurse consultants, and former defense lawyers focuses exclusively on cases like these. Led by Tommy Hastings, who is board-certified in personal injury trial law, we dedicate our practice solely to medical negligence litigation. When acting as your Arizona infant delayed airway management lawyer, we understand both the medicine and the law behind neonatal respiratory injuries. We can review your child’s medical records, identify where the standard of care may have been violated, and explain your legal options at no cost.
Understanding Neonatal Resuscitation Standards and Airway Protocols
The standard of care for neonatal airway management often follows the Neonatal Resuscitation Program (NRP) guidelines, which dictate specific timelines for suctioning, positive pressure ventilation, and intubation based on the infant’s heart rate and oxygen saturation.
The NRP is a structured training and response framework developed by the American Academy of Pediatrics and the American Heart Association. It teaches delivery room teams exactly how to evaluate and respond when a newborn is not breathing adequately. These guidelines are not suggestions; they represent the minimum actions a competent medical team should take.
When a hospital staff fails to adhere to these protocols, deviations from them can form the basis of a medical malpractice claim. An infant airway negligence lawyer often begins a case investigation by comparing the medical records against these strict timelines to identify unexplainable delays that compromised the infant’s health.
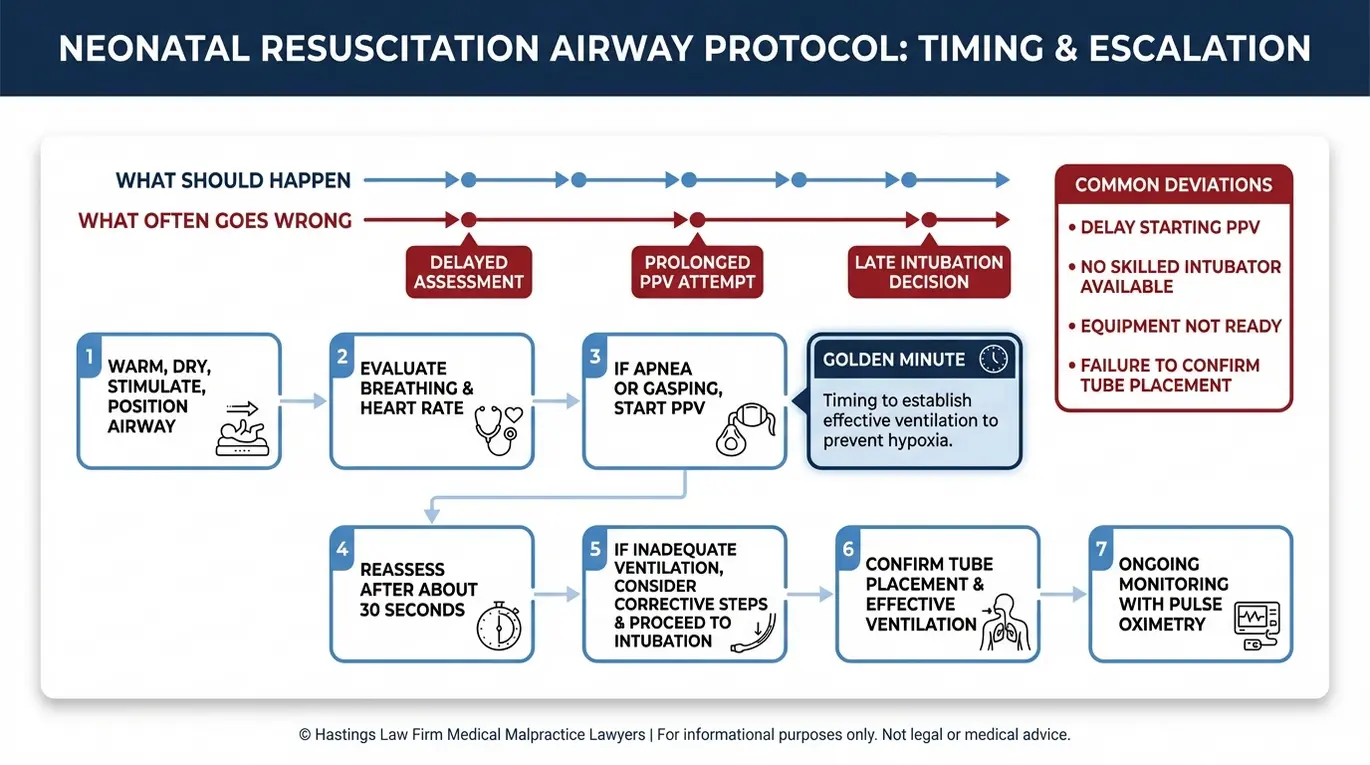
One of the most critical concepts in neonatal resuscitation is the “Golden Minute.” This window refers to the first 60 seconds after birth during which the care team must assess the infant’s breathing, heart rate, and tone. Every second counts during this window. If a child is apneic (not breathing) or gasping (struggling for air), the team cannot wait and see; they must act immediately to establish ventilation. According to a neonatal resuscitation program algorithm published in PubMed Central, the progression of interventions follows a specific, time-sensitive sequence designed to restore oxygenation before permanent damage occurs.
NRP Intervention Checklist:
- Initial steps (within the Golden Minute): Dry and stimulate the infant; clear the airway if needed; assess breathing and heart rate.
- CPAP or Positive Pressure Ventilation (PPV): If the infant is gasping or not breathing, or the heart rate falls below 100 bpm, PPV should begin immediately.
- Endotracheal intubation: If PPV does not improve heart rate within 30 to 60 seconds, or if the infant shows signs of severe respiratory failure, the team should proceed to intubation.
- Surfactant therapy: For premature infants or those with specific lung conditions, surfactant, a substance that helps keep the lungs inflated, may be administered through the endotracheal tube.
- Chest compressions: If the heart rate remains below 60 bpm after at least 30 seconds of effective ventilation, chest compressions should be initiated.
- Epinephrine: If the heart rate remains below 60 bpm despite 60 seconds of chest compressions with adequate ventilation, epinephrine should be administered.
Several clinical signs should trigger immediate escalation of airway support. Meconium aspiration syndrome, which occurs when a newborn inhales a mixture of meconium and amniotic fluid, can obstruct the airway and requires rapid intervention.
A low Apgar score, the standardized assessment given at one and five minutes after birth, can also signal that the baby is not getting enough oxygen. A score that remains low at five minutes is a major red flag indicating that resuscitation efforts are not succeeding. When these warning signs are present and the team does not act within the expected timeframe, a delayed airway management attorney can investigate whether the standard of care was met.
Distinguishing Failure to Intubate From Improper Intubation
Not all airway errors look the same, and the legal analysis depends heavily on what type of mistake occurred. There is an important distinction between a provider’s negligent decision *not* to intubate, such as ignoring clinical signs that called for it, and the negligent *performance* of the intubation procedure itself.
Providers perform endotracheal intubation (ETI) to deliver oxygen directly to the lungs. This procedure involves placing a tube, known as an endotracheal tube (ETT), into the infant’s trachea. When performed correctly, it can be lifesaving. But errors during the procedure, such as placing the tube into the esophagus instead of the trachea, failing to confirm tube placement, or causing physical trauma to the airway, can make an already dangerous situation worse. While these protocols are standard in labor and delivery units, similar failures can occur in other high-pressure environments, leading to preventable emergency room errors or NICU complications.
An infant airway negligence lawyer evaluates both categories of error. In some cases, the failure is one of omission: the team saw the warning signs but did not act. In others, it is one of execution: the team attempted to intubate but did so improperly, wasting critical time or causing additional injury. Both can constitute negligence, but proving each requires different evidence and expert testimony.
Proving Negligence in Neonatal Airway Management Cases
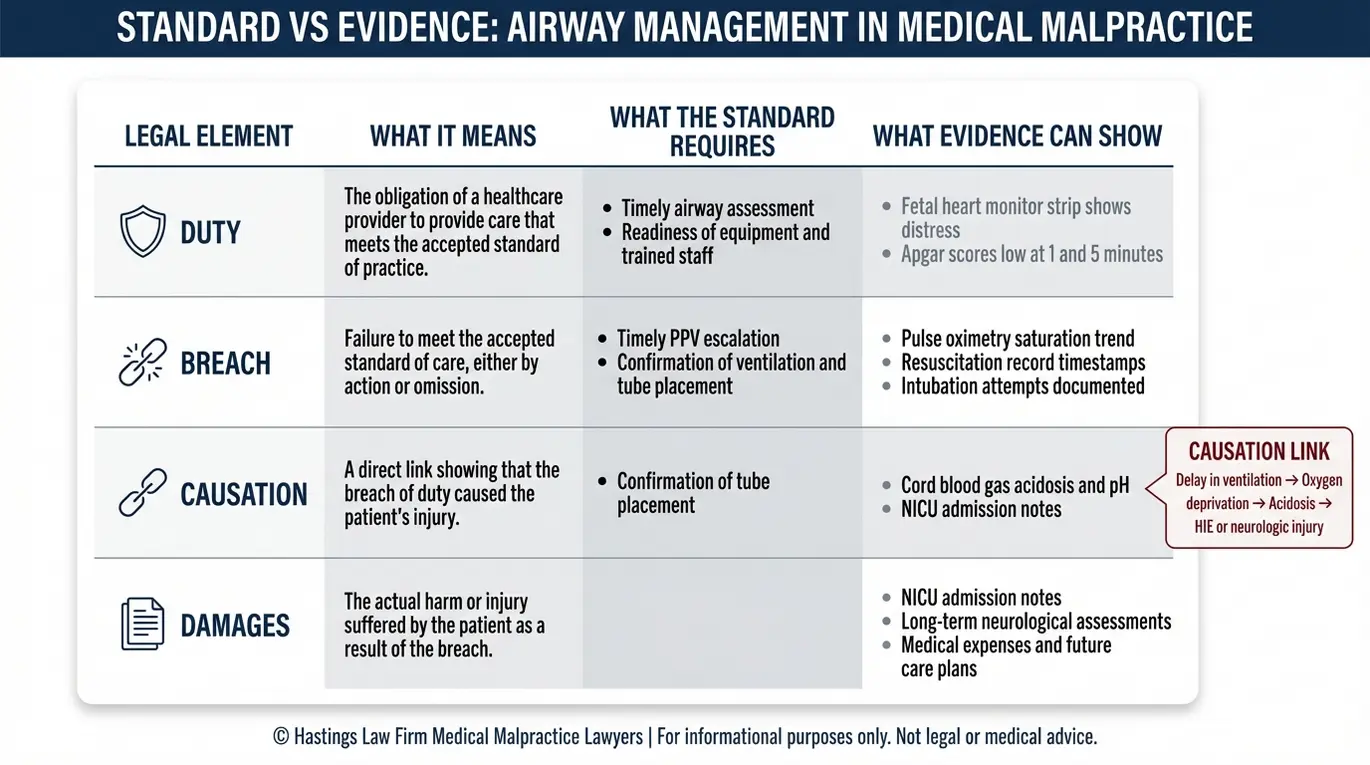
To prove negligence, a plaintiff must demonstrate that the medical provider owed a duty of care, breached that duty by failing to manage the airway according to accepted medical standards, and that this breach directly caused the infant’s hypoxic injury. Each of these elements must be supported by evidence, and each one presents its own challenges.
Establishing the Duty of Care. In a delivery room or NICU, every provider involved in the birth and immediate postnatal care owes a duty to the infant. This includes obstetricians, neonatologists, nurses, and respiratory therapists. The duty is not abstract; it is defined by the specific clinical circumstances of that delivery. A provider monitoring fetal heart tracings has a duty to recognize patterns of fetal distress and escalate care accordingly.
Identifying the Breach. A breach occurs when the provider’s actions, or inactions, fall below the accepted standard. This deviation defines medical malpractice in the context of birth injuries. In airway management cases, this might involve ignoring warning signs on the fetal heart monitor, failing to have intubation equipment prepared for a high-risk delivery, or not calling for neonatal backup when the clinical picture warranted it.
Pulse oximetry, a non-invasive method that measures the oxygen saturation in the infant’s blood through a sensor on the skin, is one of the tools we examine closely. If the data shows declining oxygen levels and the team did not respond within the expected timeframe, that gap can support a finding of negligence. A qualified lawyer for airway management errors knows how to scrutinize these electronic records to pinpoint the exact moment the breach occurred.
Proving Causation. This is often the most contested element. The defense will often argue that the injury was unavoidable, genetic, or caused by an infection rather than the delay in resuscitation. To counter this, we rely on objective clinical evidence to establish legal liability.
Umbilical cord blood gas analysis, a test that measures the pH level and base deficit in blood drawn from the umbilical cord shortly after birth, provides critical data about the degree and timing of oxygen deprivation. According to the NCBI Bookshelf resource on Cord Blood Gas, acidosis, an abnormally low pH in the blood, can confirm that the infant experienced significant oxygen deprivation around the time of delivery.
As an Arizona birth injury lawyer, our team works with qualified neonatal experts to connect the timeline of the provider’s actions to the objective lab values and imaging results. This comparison of expert testimony is crucial; we must prove that if the airway had been secured sooner, the child’s pH levels would have remained safe, and the brain injury would have been prevented. We build the case that the delay, not some other factor, caused the harm.
The Hastings Law Firm Difference
Results matter, but what truly sets us apart is how we achieve them. Every verdict, every settlement, and every Arizona courtroom victory comes from one guiding promise: To treat each client’s fight for justice as if it were our own.
This balance of skill, experience, and empathy reflects our core philosophy that justice should not only compensate the injured, but also make healthcare safer nationwide.

Consequences of Delayed Intubation and Oxygen Deprivation
Delayed intubation prevents oxygen from reaching the brain, leading to perinatal hypoxia or asphyxia, which can rapidly progress to permanent conditions such as Hypoxic-Ischemic Encephalopathy (HIE) or Cerebral Palsy.
The developing brain is extraordinarily sensitive to oxygen loss. When a newborn’s airway is not secured in time, brain cells begin to suffer damage within minutes. Birth asphyxia, the deprivation of oxygen to the infant during or immediately after delivery, triggers a cascade of cellular injury. Initially, primary neuronal death occurs due to energy failure. If oxygen is not restored quickly, the damage becomes irreversible, leading to widespread tissue necrosis. An infant asphyxia lawyer understands the medical complexity of these mechanisms and how they translate into lifelong disabilities.
Hypoxic-ischemic encephalopathy (HIE), a specific type of brain injury caused by reduced blood flow and oxygen to the brain around the time of birth, is a common outcome of these failures. A systematic review published in PubMed Central examining the relationship between neonatal HIE and long-term cognitive outcomes documents the significant link between the severity of the initial oxygen deprivation event and lasting neurological deficits. The consequences vary depending on how long the brain went without adequate oxygen and how quickly effective treatment was initiated. The severity of HIE is often graded using the Sarnat staging system, which classifies the injury as mild, moderate, or severe based on clinical presentation.
Long-term neurological consequences of delayed airway management can include:
- Cerebral palsy: A group of disorders affecting movement, muscle tone, and coordination, often caused by brain damage before, during, or shortly after birth. Severe cases may result in quadriparesis (weakness affecting all four limbs), requiring 24-hour care.
- Cognitive disabilities: Impairments in learning, memory, attention, and problem-solving that can range from mild learning differences to profound intellectual disability.
- Motor function loss: Difficulty with voluntary movements, fine motor skills, or the ability to walk independently.
- Seizure disorders: Recurrent seizures that may require lifelong medication and monitoring, which can further impact brain development.
- Vision and hearing impairment: Damage to the areas of the brain responsible for processing sensory information, such as cortical visual impairment (CVI).
The severity of these outcomes underscores why seconds and minutes matter in the delivery room. A newborn respiratory distress attorney examines the medical timeline to determine whether earlier intervention could have prevented or reduced the extent of the injury.
Reperfusion Injury After Oxygen Restoration
The harm does not always end once oxygen is restored. Reperfusion injury, a secondary wave of damage that can occur when blood flow and oxygen return to tissue that has been deprived, creates a surge of harmful molecules called free radicals. This paradoxical injury means that even after the airway is secured, the brain may continue to sustain damage if the transition is not carefully managed.
HIE is a brain injury caused by a lack of oxygen and blood flow at birth. Therapeutic hypothermia, sometimes called cooling therapy, has become a critical part of the standard of care for infants diagnosed with moderate to severe HIE. The treatment involves lowering the infant’s core body temperature to around 33.5°C (92.3°F) for 72 hours to slow the metabolic processes that drive secondary brain injury. To be effective, cooling therapy should begin within six hours of birth. If the medical team fails to initiate cooling within that window, or if the infant is not transferred to a facility equipped for the procedure in time, that delay may itself constitute a separate act of medical malpractice.
Identifying Liable Parties for Infant Respiratory Distress Injuries
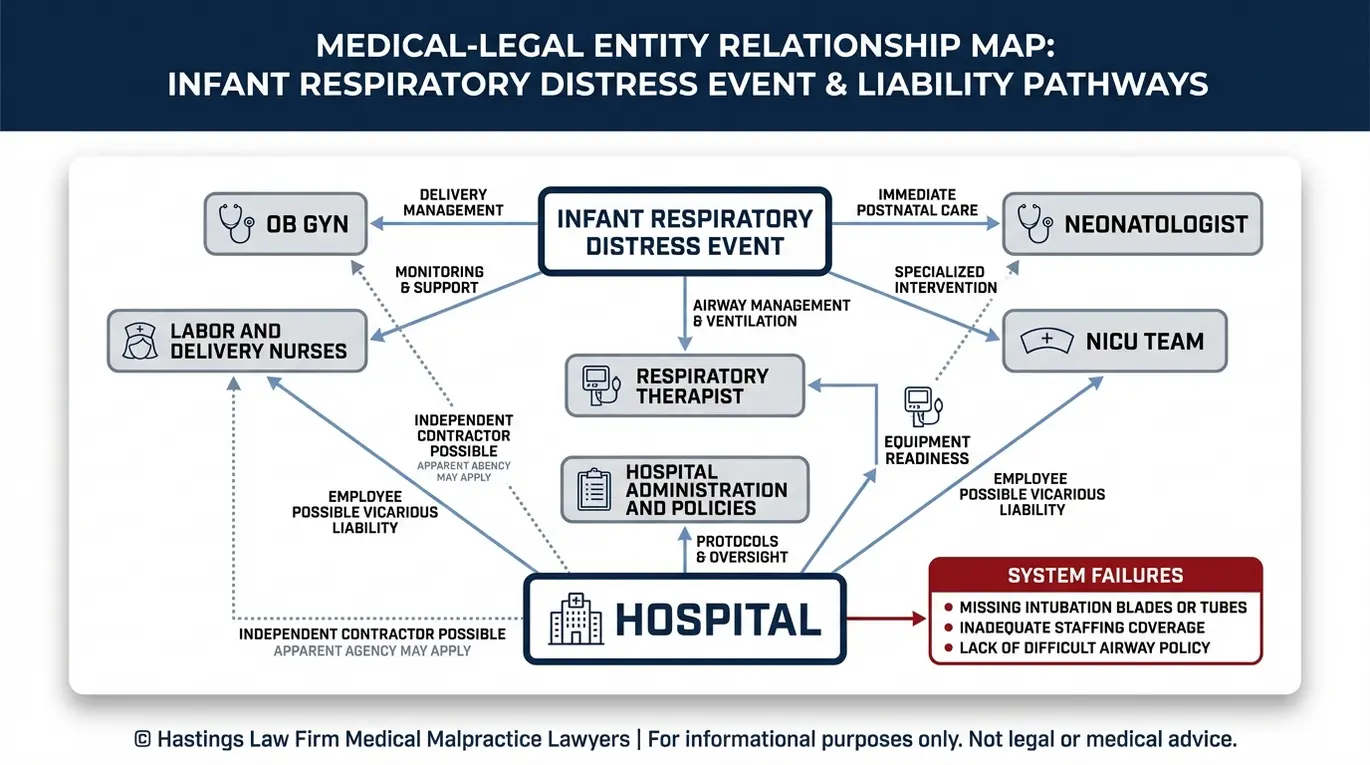
Liability for airway management errors can extend beyond the delivering obstetrician to include neonatologists, respiratory therapists, nurses, and the hospital itself for failing to maintain proper equipment or staffing levels.
Birth injury cases involving neonatal respiratory distress often reveal that the failure was not caused by a single person. Instead, it may reflect a breakdown across multiple providers and systems. As a Phoenix medical malpractice lawyer, our team investigates every level of care to identify where responsibility lies. We look for systemic issues, such as a nurse failing to escalate a concern because they were intimidated by a doctor, or a hospital failing to enforce its own chain of command policies.
Potential liable parties in neonatal airway cases:
- Obstetricians: For failing to anticipate a difficult delivery, not ordering a neonatal team to be present for a high-risk birth, or not recognizing signs of fetal distress that warranted earlier intervention.
- Neonatologists and pediatricians: For delayed response to the delivery room, failure to follow NRP protocols, or errors in performing intubation.
- Nurses and respiratory therapists: For not monitoring the infant’s status closely enough, failing to alert the physician to declining vital signs, or not preparing airway equipment in advance.
- The hospital or birthing center: For institutional failures such as inadequate staffing, missing or malfunctioning equipment (for example, unavailable intubation blades or a broken laryngoscope), or lack of policies for managing airway emergencies. In some cases, infants born in non-hospital settings are transferred to the ER, where emergency room errors can exacerbate the injury if the receiving team is unprepared.
Vicarious Liability. Even when the individual provider is an independent contractor rather than a hospital employee, the hospital may still bear legal responsibility. Under the legal doctrine of vicarious liability, which means the hospital may be responsible for the actions of its staff, a hospital can be held accountable for providers if the patient reasonably believed the provider was part of the hospital’s team.
This “apparent agency” theory is particularly relevant in hospital birth settings, where patients rarely choose or even know which neonatologist or anesthesiologist will be present. An attorney for neonatal negligence will examine employment agreements, hospital credentialing records, and billing practices to determine how liability should be allocated.
Arizona Statute of Limitations for Infant Airway Negligence Claims
In Arizona, the standard statute of limitations for medical malpractice is two years from the date of injury, but for minors, this period is “tolled,” meaning it is paused, until the child turns 18. This generally allows a claim to be filed up until the child’s 20th birthday in many cases.
The two-year filing deadline is set by A.R.S. § 12-542, which governs personal injury claims in Arizona. For adults, the clock typically starts on the date the injury occurs. But because infants cannot advocate for themselves, Arizona law provides additional time through the tolling provision for minors. This protects the child’s right to seek justice even if their parents did not file a claim immediately after birth.
Evidence is perishable. Over the course of 18 years, medical records can be lost, corrupted, or destroyed. Key witnesses, such as nurses and residents, often move to other states or retire, making them difficult to locate or depose. Memories also fade; a doctor’s recollection of a specific delivery will be much less reliable a decade later.
For these reasons, an Arizona infant malpractice attorney will generally recommend that families begin the investigation as soon as they suspect something went wrong, even if the legal deadline is technically years away. Securing the evidence now preserves the strength of the claim for the future.
Some birth injuries are not immediately apparent. A child may appear healthy at birth but later show signs of developmental delays, cognitive difficulties, or motor impairment that are ultimately traced back to oxygen deprivation during delivery. In those cases, the statute of limitations may not begin until the injury is discovered or reasonably should have been discovered. The application of this rule is fact-specific and often contested by defense attorneys, which makes early legal consultation especially important to avoid missing critical deadlines.
Recoverable Compensation for Long-Term Respiratory Injuries
Compensation in infant airway cases includes economic damages for lifetime medical care and lost earning capacity, as well as non-economic damages for pain, suffering, and loss of enjoyment of life. Because these injuries often require decades of ongoing care, the financial stakes are significant.
Economic damages cover the measurable financial losses caused by the injury:
- Past and future medical bills, including surgeries, hospitalizations, medications, and specialist visits.
- Physical, occupational, and speech therapy needed throughout childhood and adulthood.
- Attendant care and in-home nursing, which can cost millions over a lifetime.
- Adaptive equipment such as wheelchairs, communication devices, and modified vehicles.
- Lost earning capacity if the child’s disability prevents them from working as an adult. A vocational expert can project what the child likely would have earned based on family history and statistics, ensuring the settlement accounts for their loss of financial independence.
Non-economic damages address the human cost that cannot be reduced to a dollar figure:
- Physical pain and suffering endured by the child.
- Emotional distress and mental anguish.
- Loss of enjoyment of life, covering the inability to participate in normal childhood activities.
- Disfigurement or physical impairment.
- Loss of consortium, which compensates family members for the loss of companionship and the altered family dynamic.
| Damage Category | What It Covers | How It Is Calculated |
|---|---|---|
| Economic Damages | Medical costs, therapy, attendant care, lost earning capacity | Based on actual bills, expert projections, and economic analysis |
| Non-Economic Damages | Pain, suffering, emotional distress, loss of enjoyment of life | Based on the severity and permanence of the injury |
| Wrongful Death Damages | Funeral costs, loss of companionship, lost future earnings | Applicable if the infant does not survive the injury |
If the respiratory injury tragically results in the loss of the child, the family may pursue a wrongful death claim. This allows parents to recover funeral expenses and compensation for the profound loss of their child’s love and companionship.
A critical tool in these cases is the Life Care Plan. This is a detailed document prepared by medical and financial experts that projects the full cost of caring for a child with a brain injury over their expected lifetime, often spanning 50 years or more. The Life Care Plan accounts for inflation, changing medical needs, and the level of assistance the child will require at each stage of life. A lawyer for hypoxic brain injury compensation works closely with these experts to make sure no category of need is overlooked, so the family has the resources to provide the best possible quality of life for their child.
Contact the Arizona Birth Injury Attorneys at Hastings Law Firm Today for Help
No amount of money can undo the harm your child has suffered. But securing the right financial resources can make a meaningful difference in the quality of care and support your family provides for years to come.
At Hastings Law Firm, we handle these cases because we believe accountability matters, both for your family and for the families who come after you. Our team includes in-house nurse consultants and former defense attorneys who know how hospitals build their cases, and we prepare every claim from day one as though it is going to trial.
If you believe your newborn’s injury resulted from delayed airway management, we are here to help you find answers. As an Arizona infant delayed airway management lawyer, we offer a free, confidential case evaluation, and you pay no attorney fees unless we recover compensation on your behalf. Contact us today to talk about what happened and learn what options are available to your family.
Frequently Asked Questions About Infant Delayed Airway Management in Arizona

This content was researched and written by the Hastings Law Firm editorial team, which includes attorneys, medical professionals, and experienced researchers. Our writing is informed by internal knowledge and practical experience, and we cross-check critical details against authoritative sources cited throughout. Every piece undergoes human-led fact-checking and legal review. Because legal and medical information can change, if you spot an error, please contact us. Learn more about our content standards and review process on our editorial policy page.

Tommy Hastings, founder of Hastings Law Firm, is a board-certified personal injury trial lawyer dedicated exclusively to healthcare injury cases. Since 2001, he has represented injured patients and families in litigation against major hospital systems, pharmaceutical companies, and negligent healthcare providers nationwide. He has handled numerous high-profile cases that have drawn national media attention and resulted in multi-million dollar recoveries. He draws on that experience in his writing, helping readers understand how these cases work and what options may be available to them.
